
Small Incision Lenticule Extraction has become increasingly popular for the treatment of refractive errors. Today, more than 2 million SMILE surgeries for myopia and myopic astigmatism have been performed worldwide. In myopic SMILE, an intrastromal lenticule is created by the VisuMax femtosecond laser (Carl Zeiss Meditec), dissected, and then subsequently removed through a small incision. At this point, the lenticule is deemed to have served its useful purpose and is typically thrown away after surgery. That equates to 2 million discarded lenticules, which is a lot of wasted tissue.
In recent years, a number of researchers, including our own team in Italy, have been investigating whether it might be feasible to make better use of the discarded lenticules. In theory, the lenticules obtained from donor corneas could be used to insert tissue into a pathological cornea in order to potentially treat conditions such as hyperopia, presbyopia, keratoconus, ectasia, and certain corneal dystrophies.
FIRST STEPS
In 2012, the initial feasibility studies in animal models, conducted by Jodhbir S. Mehta, BSc(Hons), MBBS, FRCOphth, FRCS(Ed), FAMS, and colleagues at the Singapore National Eye Institute, demonstrated that lenticules could be successfully cryopreserved and re-implanted in animals with a high degree of safety.1 The results led some to hypothesize that lenticules could be reused to correct refractive errors in other eyes, and preliminary reports were published on the implantation of myopic lenticules to treat hyperopia and presbyopia.2-4
The work at our research center in Italy has focused primarily on the possibility of using implanted lenticules to reshape and stabilize the corneas in eyes with progressive keratoconus. The basic idea is to implant the lenticules intrastromally in order to improve the geometrical quality of pathological corneas affected by keratoconus (Figure 1).

Figure 1. Drawing depicting the SLAK procedure: The negative meniscus-shaped lenticule is implanted intrastromally to improve the geometrical quality of keratoconic corneas.
The procedure entails implanting a negative meniscus-shaped lenticule that is thinner in the center and thicker in the periphery—the geometric opposite of a myopic lenticule. Implanting a myopic lenticule will not work, as it increases the tissue volume in the center of the cornea where the apex of the cone is located and further steepens the corneal curvature. Implanting a negative meniscus-shaped lenticule theoretically leads to augmentation in thickness and central corneal flattening similar to the arc-shortening effect achieved with intrastromal corneal ring segments. This is achieved by placing the thickest part of the lenticule in the mid-periphery of the cornea.
Our first ex vivo study was published in 2016.2 In that study, we used 12 stromal hyperopic lenticules created by the VisuMax femtosecond laser and evaluated them with OCT and topography after they were implanted into a pocket created by a femtosecond laser. The results were positive, showing that implantation of the lenticules was a feasible and reproducible technique to achieve central corneal flattening and increased thickness. We then repeated the same technique in a model of keratoconus-shaped corneas and successfully improved the curvature and corneal thickness in the pathologic models as well.
HUMAN TRIALS
We then tested the procedure, called stromal lenticule addition keratoplasty (SLAK), in 10 patients with advanced keratoconus.3 The 6-month results confirmed our earlier results in donor corneas and was shown to clinically efficiently improve the corneal shape and regularity in all patients with keratoconus. SLAK significantly improved the mean uncorrected and corrected distance visual acuity, and OCT scans confirmed a statistically significant increase in the thickness of the central and mid-peripheral cornea produced by the lenticule implantation.
The complication rate was extremely low with SLAK, and there was no incidence of graft rejection in any eyes. It is well known that lamellar keratoplasty has a very low risk of stromal rejection, so these patients do not need long-term steroid therapy after lenticule implantation.
We have used the SLAK technique to date in 32 patients, and we have up to 18 months of follow-up (Figure 2). Thus far, the results are very promising—even more so when one considers that the alternative for these advanced keratoconus patients was an invasive penetrating or deep lamellar keratoplasty. The concept of SLAK is to offer minimally invasive surgery that is efficient and reproducible. We believe that every technique that aims to compete with the gold standard should be not only efficient but also reproducible and within the scope of all surgeons’ abilities.
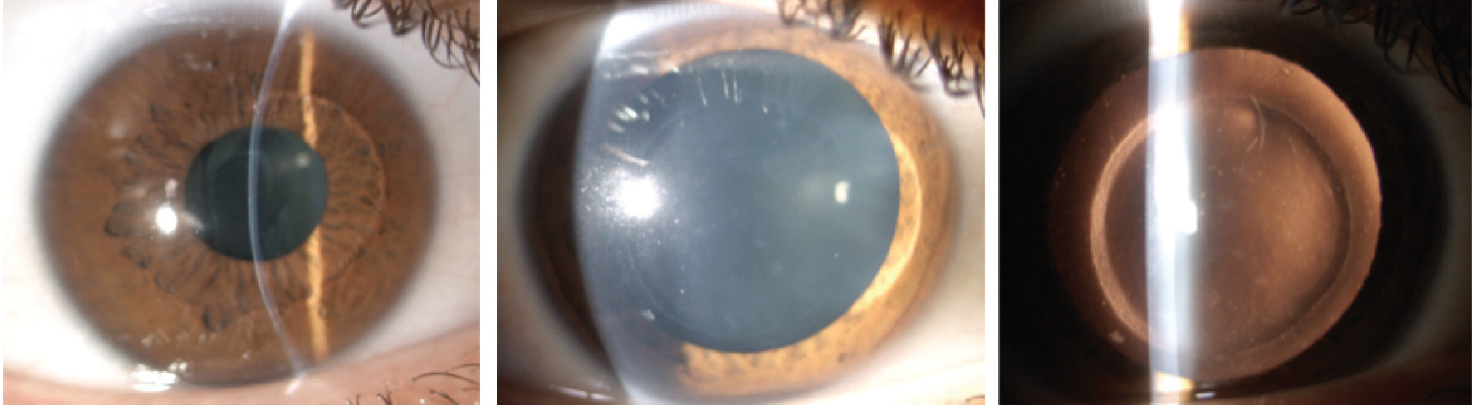
Figure 2. SLAK in advanced keratoconus: The stromal interface transparency was stable over 18 months of follow-up (left to right).
SLAK surgery is not that technically difficult to perform. The stromal pocket in which the lenticule is implanted is easily created with a femtosecond laser, and it only takes a few seconds to create. The lenticule is then sculpted in the donor cornea with the exact shape, size, and geometry required using the VisuMax femtosecond laser, and it is extracted for implantation.
With the eye under topical anaesthesia, the lenticule is implanted through the stromal incision in the pocket. Once in place, the lenticule is distended and centered on the apex of the cornea according to the topography. The entire procedure takes about 3 to 4 minutes, and patients wear a contact lens for 1 day postoperatively. They are free to return to normal activities within 2 to 3 days of surgery—it truly merits the term minimally invasive surgery.
LESSONS LEARNED
A few key points about SLAK are worth noting. First, the best visual acuity outcomes were obtained in the less-advanced keratoconus cases. This is logical if one considers that flattening a cone in the eyes of advanced keratoconus patients usually only brings them back to a moderate disease level, so their visual acuity is still severely compromised by corneal steepening. However, treating a patient with moderate keratoconus and obtaining 40% improvement in his or her curvature brings the patient closer to normal levels of curvature and, therefore, better visual acuity. The key lesson is that the earlier we can intervene in the disease process, the better the outcomes will be.
This is not to suggest, of course, that we should treat patients who can tolerate a contact lens at the very early stages of keratoconus. If a patient has 20/20 visual acuity with a contact lens and is happy with that solution, then we do not propose any kind of surgery. However, most patients do not see well with spectacles and cannot tolerate contact lenses, or they become intolerant at a later stage and will seek other solutions if their keratoconus is progressing.
WHAT IS SLAK?
Stromal Lenticule Addition Keratoplasty entails implanting a negative meniscus-shaped lenticule that is thinner in the center and thicker in the periphery—the geometric opposite of a myopic lenticule—to reshape and stabilize the corneas in eyes with progressive keratoconus.
The basic idea of SLAK surgery is to implant the lenticules intrastromally in order to improve the geometrical quality of pathological corneas affected by keratoconus.
COMBINED WITH CXL
Going forward, another potentially interesting application of SLAK will be in combination with CXL, a proven and widely used modality to improve the tensile strength of the cornea and halt the progression of keratoconus. The idea would be to use CXL to lock in the strong results of the reshaping that have already been achieved with the lenticule implantation.
Lenticule implantation could also be performed in patients with progressive keratoconus and very thin corneas that are below the safety margin for CXL. Performing SLAK in these patients would create sufficient thickening in the thinnest part of the cornea, enabling them to become eligible for CXL. It is these patients who are likely to derive the maximum benefit from SLAK since they cannot undergo CXL, their keratoconus is progressing, and they are facing penetrating or lamellar keratoplasty in the near future. By performing SLAK, we make the patient suitable for CXL, delay or halt their keratoconus progression, and improve their vision as well.
Likewise, SLAK may also benefit patients who are contact lens intolerant and who may require keratoplasty in the near future. Improving their corneal curvature by around 30% to 40% may enable them to wear a contact lens once again and avoid the need for invasive graft surgery. With this minimally invasive approach, we potentially have a wide range of positive effects for many different categories of patient.
The promise of lenticule implantation is exciting, but much remains to be done to bring this technique into mainstream practice. Therefore, we recently established an international research group, whose members include many renowned surgeons in the field of cornea, such as Harminder Singh Dua, CBE, FRCS (UK); Béatrice Cochener, MD, PhD (France), Jorge L. Alió, MD, PhD and Jorge L. Alió del Barrio (Spain), Josè L. Guell, MD, PhD (Spain), Jodhbir S. Mehta, BSc(Hons), MBBS, FRCOphth, FRCS(Ed), FAMS (Singapore), and our own team in Italy.
The goal is to pool research in this developing field, avoid single-center bias, perform multicenter trials, and set standards and protocols for the technique of lenticule implantation for the benefit of the wider ophthalmological community. Another broad aim of the group will be to promote the creation of a European eye bank to preserve tissues and lenticules donated by refractive surgery patients that could be processed and certified for eventual clinical use.
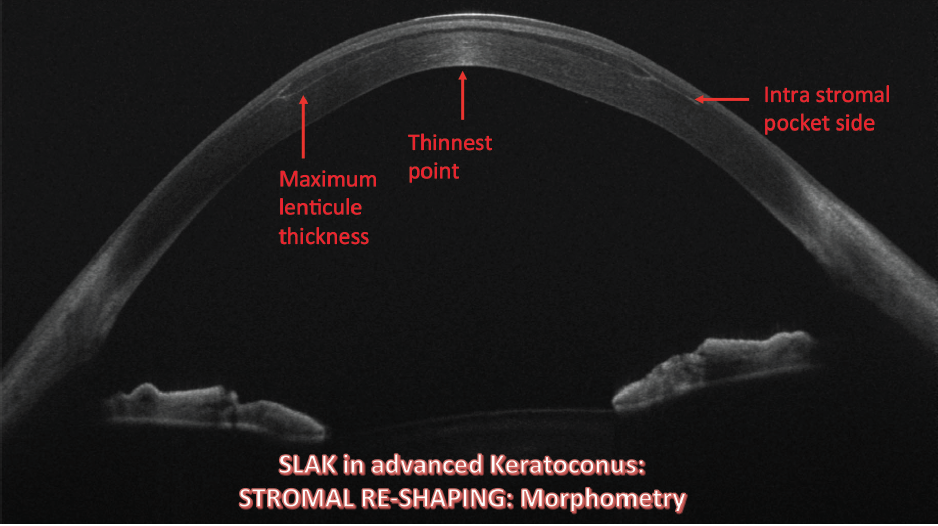
Figure 3. Widefield swept source OCT scan revealing that the lenticule was correctly placed inside the pocket with a peripheral bulging of the anterior and posterior surface.
CONCLUSION
Although it is still early and more studies with longer follow-up are needed, the SLAK procedure has been shown to be safe and clinically efficient in improving the corneal shape (Figure 3) and vision in patients with keratoconus.
Explore more and get in contact!
1. Angunawela RI, Riau AK, Chaurasia SS, Tan DT, Mehta JS. Refractive lenticule re-implantation after myopic ReLEx: a feasibility study of stromal restoration after refractive surgery in a rabbit model. Invest Ophthalmol Vis Sci. 2012;53:4975-4985.
2. Ganesh S, Brar S, Rao P, et al. Cryopreservation of extracted corneal lenticules after small incision lenticule extraction for potential use in human subjects. Cornea. 2014;33:1355-1362.
3. Sun L, Yao P, Li M, Shen Y, Zhao J, Zhou X. The safety and predictability of implanting autologous lenticule obtained by SMILE for hyperopia. J Refract Surg. 2015;31:374-379.
4. Lim CH, Riau AK, Lwin NC, Chaurasia SS, Tan DT, Mehta JS. LASIK following small incision lenticule extraction (SMILE) lenticule re-implantation: a feasibility study of a novel method for treatment of presbyopia. PLoS One. 2013;8:1-12.
5. Mastropasqua L, Nubile M. Corneal thickening and central flattening induced by femtosecond laser hyperopic-shaped intrastromal lenticule implantation. Int Ophthalmol. 2016;37:893-904.
6. Mastropasqua L, Nubile M, Salgari N, Mastropasqua R. Femtosecond laser-assisted stromal lenticule addition keratoplasty for the treatment of advanced keratoconus: a preliminary study. J Refract Surg. 2018;34(1):36-44.




