




Cataract surgery has an excellent safety profile. When mild or severe complications occur, however, it can be a wise decision to obtain a second opinion.
REASONS TO OBTAIN A SECOND OPINION
Reassurance. The occurrence of a complication can undermine the surgeon-patient relationship. If the outcome differs from their expectations, patients may experience fear and confusion. The simple act of obtaining a second opinion may put the patient at ease. If a second intervention is required, the patient may also appreciate the offer and prefer to have another surgeon perform the procedure. Having that colleague confirm the appropriateness of the original management plan can reassure the patient.
Experience. Sometimes, especially for young surgeons, advice from a colleague who has more experience with procedures such as IOL explantation or piggyback IOLs may be useful. Alternatively, it may be necessary to refer the patient to a colleague with subspecialty skills. For instance, laser vision correction may be required to address a refractive surprise.1-3
Not all complications require treatment, and a second opinion from an experienced colleague may be helpful in making this determination. The decision whether to intervene surgically to address a malpositioned IOL, for example, depends on the patient’s age, signs and symptoms, comorbidities, and potential for visual recovery (for more on management of malpositioned IOLs, see “IOL Complications"). If surgery is indicated, the approach depends on the type and position of the IOL and on the status of the capsular bag. Options include IOL repositioning and exchange.4 (For more on these subjects, see “Indications for IOL Exchange,” and “When to Exchange a Presbyopia-Correcting IOL and What to Put in Its Place".) Pseudophakic dysphotopsia is another complication that can sometimes be managed conservatively.5
A DIFFICULT DIAGNOSIS
A patient may be unhappy after cataract surgery despite careful preoperative management and seemingly uneventful surgery. A colleague may be able to detect subtle findings that were missed during prior examinations.6 Postoperative complications require a careful differential diagnosis. For example, the diagnosis of uveitis-glaucoma-hyphema syndrome may be missed if the classic triad is absent and there are no clear causative agents.
When dealing with a dissatisfied patient, it can be helpful to collect and review previous records and to reexamine the case from the start (see Managing Patients Unhappy With Their Vision After Refractive Cataract Surgery). Did preoperative management include a misstep? Was there an undetected contraindication for a premium IOL?
Managing Patients Unhappy With Their Vision After Refractive Cataract Surgery

Managing patients who are unhappy with their vision after refractive cataract surgery can be daunting. Patients with unsatisfactory refractive outcomes, suboptimal vision quality, and low-light dysphotopsias have issues that should be addressed. The IOLs used to treat astigmatism and presbyopia feature advanced optics that balance compromises, and patients receiving these IOLs have high expectations.
It is helpful to remember that a limited number of etiologies cause most postoperative visual complications and complaints. Two flowcharts I created organize my thought process and facilitate a systematic and thorough approach to managing these patients. Although they are not exhaustive, these flowcharts have help me to determine quickly how to proceed.
The postoperative management flowchart helps me to differentiate between a medical and a refractive etiology (Figure 1). The postoperative refractive error flowchart helps me to determine how to approach a postoperative refractive error (Figure 2). In both flowcharts, the blue diamonds pose key questions to ask, and the brown boxes show the diagnoses and treatment approaches.
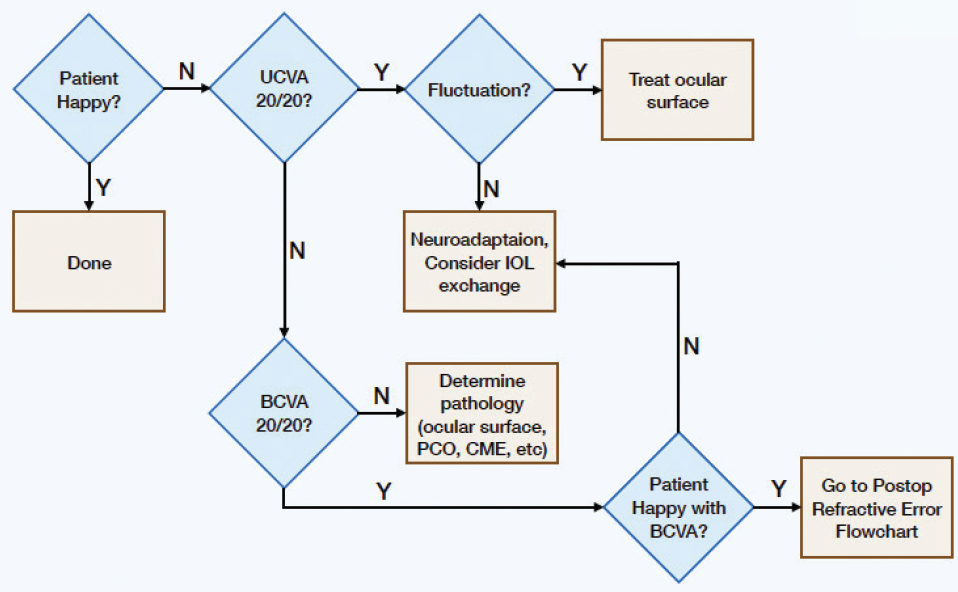
Figure 1. Postoperative management flowchart.
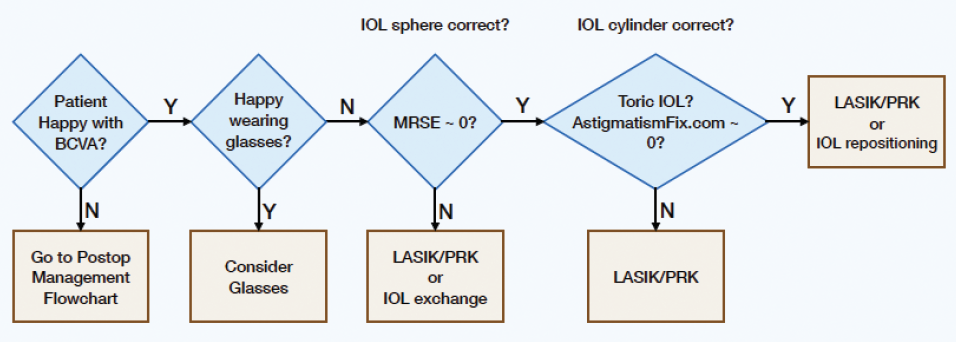
Figure 2. Postoperative refractive error flowchart.
CONCLUSION
If the clinician cannot detect the cause of a patient’s dissatisfaction, if the surgeon does not have the skills to treat a particular condition, or if the patient becomes distrustful, it can be worthwhile to seek a second opinion. In short, whenever the surgeon and/or the patient does not fill comfortable with the diagnosis and/or the treatment, seeking a second opinion should be considered. A colleague may be able to share valuable insight, confirm the proposed management plan, or offer the patient other options.
1. Durr GM, Ahmed IIK. Intraocular lens complications: decentration, uveitis-glaucoma-hyphema syndrome, opacification, and refractive surprises. Ophthalmology. Published online July 8, 2020. doi:10.1016/j.ophtha.2020.07.004.
2. Ashena Z, Maqsood S, Ahmed SN, Nanavaty MA. Effect of intraocular lens tilt and decentration on visual acuity, dysphotopsia and wavefront aberrations. Vision (Basel). 2020;4(3):1-15.
3. Kim HK, Shin JP. Capsular block syndrome after cataract surgery: clinical analysis and classification. J Cataract Refract Surg. 2008;34:357-363.
4. Schena LB. When lenses go wrong: tips on IOL explantation. EyeNet. July/August 2010. Accessed March 6, 2021. https://www.aao.org/eyenet/article/when-lenses-go-wrong-tips-on-iol-explantation
5. Tester R, Pace NL, Samore M, Olson RJ. Dysphotopsia in phakic and pseudophakic patients: incidence and relation to intraocular lens type. J Cataract Refract Surg. 2000;26:6:810-816.
6. Devgan U. Give the first surgeon the benefit of the doubt. October 15, 2019. Accessed March 6, 2021. https://www.healio.com/news/ophthalmology/20191015/give-the-first-surgeon-the-benefit-of-the-doubt