
Sponsored by Carl Zeiss

ALEX J. SHORTT, MB BCh, MSc, PhD
Consultant Ophthalmic Surgeon, The Harley Street Eye Clinic and the Optegra Eye Hospital London.
Case History
A 45-year-old man presented with visually disabling glare and blurred vision secondary to corneal scarring from episodes of herpes simplex keratitis in his left eye. UCVA and BCVA in this eye were 6/19 and 6/12, respectively, and the refraction in this eye was -1.00 -0.75 X 128º. With a rigid gas permeable (RGP) contact lens, he could be corrected to 6/7.5; however, the patient was atopic and was unable to tolerate contact lens wear.
Slit-lamp examination showed superficial corneal scarring affecting the central and inferotemporal cornea (Figure 1). Pentacam (Oculus) imaging showed mild thinning inferotemorally corresponding with the geometric center of the scar.
Therapeutic strategy
A two-step treatment strategy was used to address the superficial corneal opacity and irregular corneal shape, with 8 weeks between treatment steps. Prophylaxis against herpes simplex reactivation was added to the routine postoperative regimen after each step.
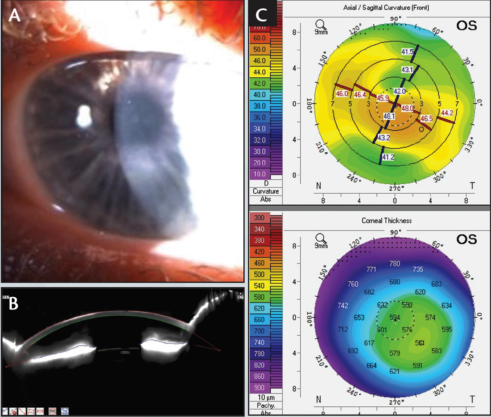
Figure 1
Step No. 1: Transepithelial PTK with the MEL 90 excimer laser (ZEISS). The opacified corneal stroma was ablated in the optical axis, and the compensatory thickening of the corneal epithelium over the thinned area of the central scar was used as a masking agent to minimize ablation at the thinnest point. The 55-μm, 9-mm transepithelial PTK resulted in epithelial breakthrough and stromal ablation over the steepest, central part of the cornea but not over the entire area of the scar.
A series of further 10-μm PTKs were performed without any masking agent, until stromal ablation was observed in all areas except in the 1.5-mm diameter zone that corresponded to the thinnest point on the Pentacam scan and to the geometric center of the scar. In the final 10-μm PTK, balanced saline solution was used as a masking agent to polish any localized irregularities.
Eight weeks after the first treatment, the patient’s subjective glare had completely resolved and UCVA and BCVA in his left eye improved to 6/15 and 6/7.5, respectively, with a refraction of +0.50 -3.75 X 80º. The corneal scarring was significantly reduced, particularly over the visual axis (Figure 2), and Pentacam imaging showed a more regular corneal shape. Despite a slight change in the corneal thickness profile, the anterior corneal shape was more regular and the apex more central.
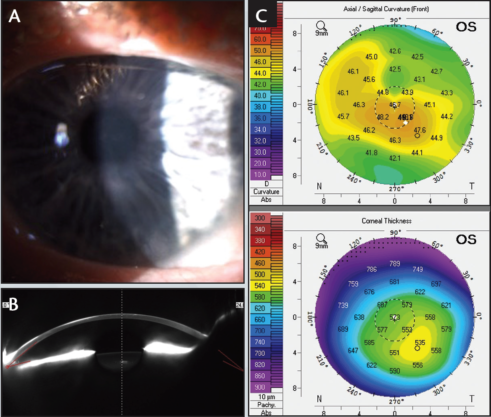
Figure 2
Step No. 2: Topography-guided correction of irregular astigmatism with the MEL 90. The aim of the second step of the treatment was to produce a spherotoric anterior stromal surface.
The ATLAS 9000 and CRS-Master software (both ZEISS) were used to plan the topography-guided treatment. After acquisition on the ATLAS 9000, corneal topography scans (Figure 3A) were imported into the CRS-Master treatment planning software (Figure 3B), and a topography-guided ablation was chosen.
The CRS-Master provides several functions to simulate the predicted treatment effect, such as postoperative corneal curvature prediction and target elevation in reference to the Best Fit Sphere. These features are intuitive and helpful in optimizing the final therapeutic laser treatment. During surgery in this patient, the the epithelium was removed by performing a transepithelial PRK to a depth of 55 μm. The topography-guided treatment was then applied to the exposed stroma, and mitomycin-C 0.02% was applied for 20 seconds.
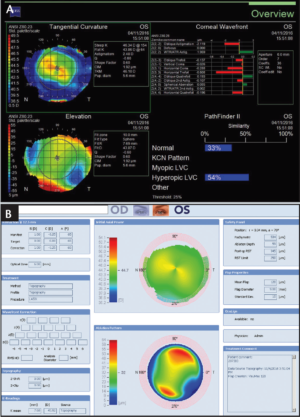
Figure 3
Final outcome
Three months after the topography-guided treatment, the patient’s UCVA and BCVA in his left eye were 6/7.5 and 6/5, respectively, with a refraction of +1.50 -1.50 X 95º). The corneal shape had improved significantly (Figure 4), and the patient reported that the glare had completely resolved and that he was extremely satisfied with his outcome.
The result in this case demonstrates that a two-step therapeutic treatment approach (transepithelial PTK followed by a topography-guided transepithelial PRK) with the MEL 90 excimer laser can result in excellent visual rehabilitation in superficial corneal scarring.
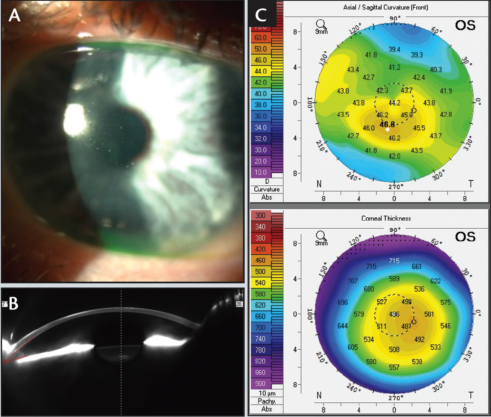
Figure 4