Discussion of Clinical Outcomes With an ERV IOL

The average eye has approximately 2.00 D of chromatic aberration for wavelengths between 400 and 700 nm and 0.80 D for wavelengths between 500 and 640 nm.1 Because corneal chromatic aberration causes blur and reduction in contrast sensitivity, the correction of this aberration by means of an IOL based on achromatic optical technology should result in a sharper focus of light. The goals of extended range of vision and extended depth of focus IOL technologies—to provide patients with enhanced contrast sensitivity and to generate an extended range of vision or depth of focus—reflect this need to compensate for corneal chromatic aberration.
AT A GLANCE
• The small difference in mean binocular decimal distance UCVA between the micro-monovision and no monovision groups groups demonstrated an ability of the Symfony IOL to tolerate refractive error.
• In the CONCERTO study, the Tecnis Symfony IOL provided visual restoration after cataract surgery with excellent visual outcomes across all distances.
• Patients enrolled in the study had minimal levels of disturbing photic phenomena and high levels of spectacle independence and postoperative satisfaction.
The ability of a diffractive IOL with achromatic technology to compensate for corneal chromatic aberration, and, thus, to enhance contrast sensitivity, has been demonstrated in previous studies.2,3 Specifically, when correction of chromatic aberration is combined with correction of spherical aberration, the retinal image quality has been shown to improve without negatively affecting depth of focus.2
ACHROMATIC DIFFRACTIVE PATTERN
With its proprietary achromatic diffractive echelette design,4 the Tecnis Symfony IOL (Abbott Medical Optics) is based on these optical principles. The achromatic diffractive pattern of this extended range of vision (ERV) IOL, which is available in both nontoric and toric versions, elongates the depth of focus of the eye and compensates for the chromatic aberration of the cornea. Therefore, this IOL does not show similar focus characteristics to either monofocal or multifocal IOLs. Clinical data do not demonstrate the typical behavior that results from designs using multiple focal points, as this ERV lens instead has an elongated focal area.
MULTICENTER STUDY
A prospective international multicenter study, the CONCERTO study, was designed to evaluate clinical outcomes obtained with the Tecnis Symfony IOL. At 40 active study sites in Finland, France, Germany, Norway, Spain, Sweden, and the United Kingdom, a total of 476 patients were enrolled and bilaterally implanted with the Tecnis Symfony IOL. Postoperative follow-up examinations were performed at 4 to 8 weeks and 4 to 6 months after second-eye surgery. The study is ongoing; to date, the 4-to-8-week clinical data are available for 290 patients.
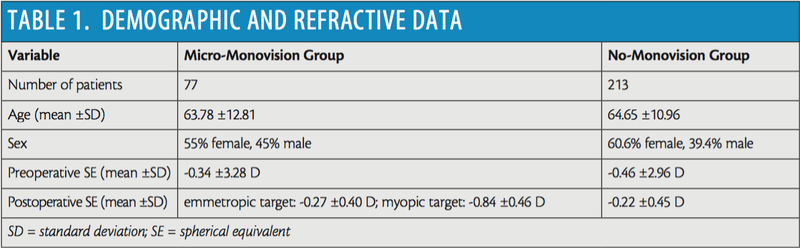
Patients were divided into two groups depending on whether monovision was intended or not: the micro-monovision group, consisting of 77 patients, and the no-monovision group, consisting of 213 patients (Table 1).
Mean binocular decimal distance UCVA was 0.93 and 0.98 in the micro-monovision and no-monovision groups, respectively (Figure 1). This outcome appears to confirm the ability of the Tecnis Symfony ERV IOL to successfully restore distance visual function. The relatively small difference between the two groups also demonstrates an ability of this lens to tolerate refractive error.
An excellent visual outcome was also observed for intermediate distance at 70 cm, with mean decimal intermediate UCVA of 0.85 and 0.77 in the micro-monovision and no-monovision groups, respectively (Figure 1). These values are similar to or better than those obtained with multiple types of multifocal IOLs, including diffractive bifocal and trifocal IOLs.5,6 Furthermore, the intermediate visual outcome obtained with the Tecnis Symfony was better than the outcomes reported for rotationally asymmetric refractive multifocal7 and apodized diffractive IOLs.8
Near decimal UCVA outcome at 40 cm was 0.77 and 0.66 in the micro-monovision and no-monovision groups, respectively (Figure 1). These values are similar to those reported for some models of multifocal IOLs, including refractive7 and diffractive.6 Law and colleagues9 recently reported a mean binocular decimal near UCVA value of 0.7 in a group of eyes implanted with a trifocal diffractive IOL model.





In agreement with these visual outcomes, the level of spectacle independence achieved with the Tecnis Symfony IOL was high, with most of the eyes not requiring spectacles for any distance, intermediate, or near visual activity (Figure 2). The micro-monovision option provided better outcomes in terms of spectacle independence, with less than 10% of eyes needing glasses for near activities.
As expected considering the design of the IOL, the levels of certain types of photic phenomena were minimal. More than 88% of patients reported no or mild halos, glare, starbursts, and other types of photic phenomena (Figure 3). This is in contrast with dissatisfaction rates and patient complaints reported with other presbyopia-correcting IOLs, for which medium or greater difficulties were reported by 33.7% (glare) and 66.7% (halos) of patients at 3 months postoperative.9
Finally, patient satisfaction, both with visual outcomes and with the procedure, was high. On a scale from 0 (not at all satisfied) to 10 (very satisfied), mean scores of patient satisfaction with distance, intermediate, and near vision were 8.75, 9.18, and 8.53 in the micro-monovision group, and 8.91, 8.92, and 7.76 in the no-monovision group, respectively (Figure 4). These values demonstrate high levels of satisfaction among both groups of patients in this study.
Additionally, more than 94% of patients reported that they would recommend the same procedure to their friends and family, and up to 96% would choose the same lens again. Likewise, surgeon satisfaction with regard to handling and performance of the lens and achieving target refraction were also high (Figure 5).
CONCLUSION
In the CONCERTO study, the Tecnis Symfony IOL provided visual restoration after cataract surgery with excellent visual outcomes across all distances. These visual results were associated with minimal levels of disturbing photic phenomena and high levels of spectacle independence and postoperative patient satisfaction.
Ready to Claim Your Credits?
You have attempts to pass this post-test. Take your time and review carefully before submitting.
Good luck!
Recommended
- Cataract Surgery
More Than 20 Radial Keratotomy Incisions
Audrey Rostov, MD; Jorge L. Alió, MD, PhD, FEBOphth, FWCRSAudrey Rostov, MD; Jorge L. Alió, MD, PhD, FEBOphth, FWCRS

