
In my clinic at the Anterior and Refractive Surgery Department of the Rothschild Foundation in Paris, I have followed thousands of cases of keratoconus over the past 15 years, as well as patients who do not yet have a diagnosis of keratoconus but who, I believe, rub their eyes too much. I consider excessive eye rubbing to be the root cause of keratoconus.
Whatever is causing patients to rub their eyes—allergies, dry eye disease (DED), blepharitis, or something else—it is our responsibility as clinicians to identify it and help them stop the behavior, even during sleep. With the goal of getting to the root-cause of patients’ eye rubbing, as part of our comprehensive slit-lamp examinations on all keratoconic patients, my team and I inspect the eyelids and lash line. It is logical that if the health of the lid margin is poor, then the patient would feel itching and/or discomfort and rub their eyes more frequently. The purpose of our examination is to make the differential diagnosis between Demodex blepharitis, non-Demodex blepharitis, and meibomian gland dysfunction (MGD). We specifically look for signs of Demodex, such as crusting and collarettes—the pathognomonic sign of this infestation.1,2
The Connection Between Keratoconus and Demodex
Demodex blepharitis is easy to miss, because its symptoms overlap with those of other ocular surface diseases.1 Yet, Demodex blepharitis is very easy to diagnose with just a slit lamp, simply by having the patient look downward and identifying collarettes along the base of the superior lash line (see the sidebar, Identifying Demodex Blepharitis at the Slit Lamp). Once we began looking for the clinical signs of Demodex, we found it—not only in our patients with keratoconus, but in our refractive population as well. It has been most prevalent in the eyes of people who complain of ocular fatigue, discomfort, and/or sensations of burning and itching.
Identifying Demodex Blepharitis at the Slit Lamp
Ask your patients to look down to ensure you can examine the base of the lashes.
Photos courtesy of Marc Bloomenstein, OD
Clinical Screening for Demodex Blepharitis
Again, it is easy to find collarettes and crusting along the superior lash line at the slit lamp. We start by asking the patient to look down toward the floor. Then, we look at the eyelids and lashes, checking both the anterior and posterior eyelid margin for inflammation. We also examine the superior part of the eyelid at the lash line. Additionally, we interview the patient about their symptoms. We ask, when do their eyes feel itchy? When do they catch themselves rubbing their eyes? What are their sleep habits?
Usually, the itchiness associated with Demodex blepharitis occurs along the upper eyelid; patients rubbing their eyes in a horizontal direction is a telltale sign. It has no specific time of day; it is more generalized and frequently turns to a burning sensation. In contrast, rosacea tends to flare at certain times of the day and is sensitive to environmental factors like air conditioning. With blepharitis, patients often rub the nasal side of their eyes, because blepharitis frequently includes meibomian gland dysfunction (MGD).
It is now the standard in our clinic to look for Demodex in all eyes with mild blepharitis, and I encourage all practitioners to do the same. In its early stages, before the patient becomes very symptomatic, Demodex often has similar signs as other ocular pathologies, such as DED and MGD.3 I also believe Demodex blepharitis is more prevalent in people who have rosacea.1
Case Study: Demodex Blepharitis Found in Eye With Keratoconus
Elizabeth Yeu, MD
A 30-year-old White male living in South Carolina, USA underwent LASIK in 2015 by a prominent, meticulous surgeon there. The patient later moved to Atlanta, by which time his UCDVA had regressed in both eyes, although worse in the right. In 2019, he sought an evaluation for a LASIK enhancement with the original doctor, during which he was told that he had keratoconus in the right eye that would require treatment with corneal crosslinking (CXL). He underwent the CXL procedure that same year.
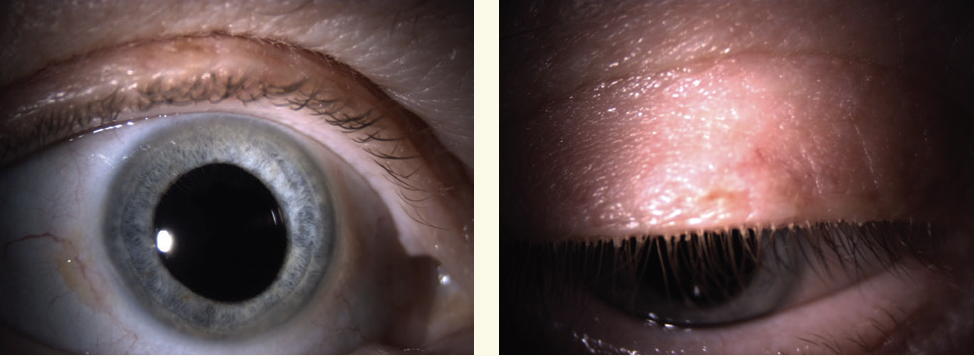
When he presented to my office in 2022 for evaluation for a LASIK enhancement, his UCVA was 20/20 OS and 20/60 OD (Figure 1). He complained of blurred vision, particularly in the right eye, and he admitted to rubbing his eyes “a lot,” especially in the morning, because they itched. He thought the itching was located “across my eyelids." The patient reported having no history of seasonal or perennial allergies.
My examination revealed Demodex collarettes along the lash line of both eyes—grade 3 on the left eye and grade 4 on the right eye. There were misdirected lashes, more along the left eyelids. The lower lids showed mild erythema bilaterally, with 1+ telangiectasis and turbid meibum that was moderately difficult to express. There was a mild mixed papillofollicular reaction of the upper palpebral conjunctiva. The LASIK flaps were well-centered and clear, without punctate epitheliopathy. The rest of the anterior segment examination was unremarkable.
This patient experienced no relief from antihistamines or montelukast because his symptoms were due to Demodex blepharitis, and his eye rubbing (worse OD) led to the post-LASIK ectasia. Although CXL can help slow the progression of keratoconus and post-LASIK ectasia, its effectiveness will be compromised if the eye continues to experience repeated microtrauma from frequent eye rubbing.
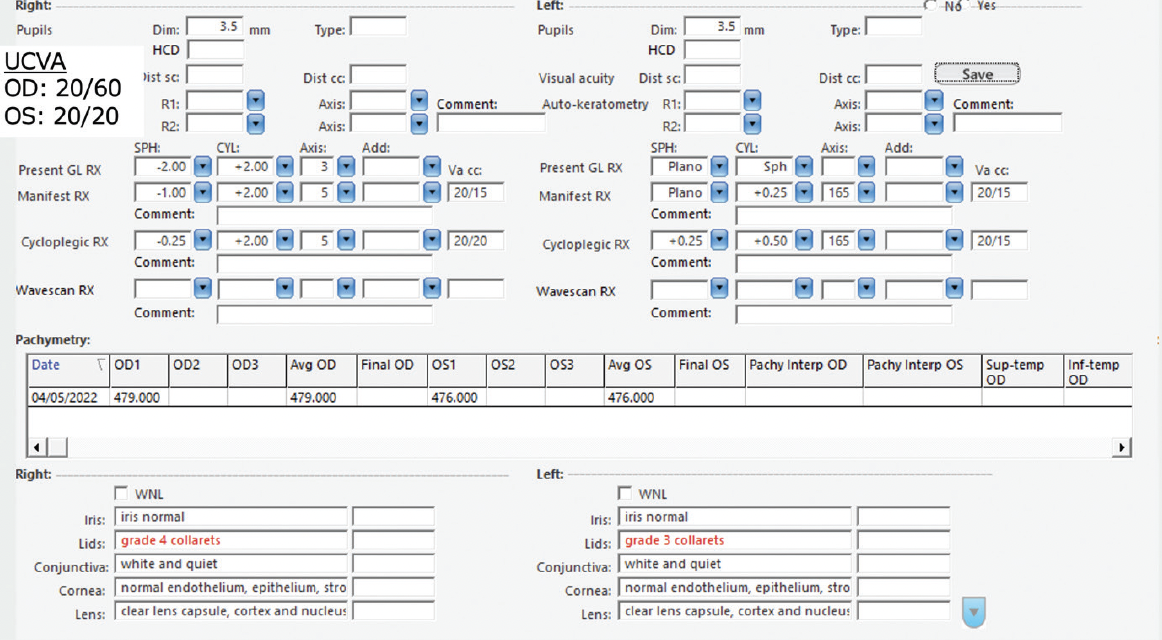
Figure 1. A preoperative examination in 2022 of this patient, who complained of rubbing his eyes due to itchiness, revealed collarettes along the lash line of both eyes.

Figure 2. In placido topography images of the right (A) and left (B) eyes, the axial map images (upper left box of each 4-image display) show well-centered, flat topographic beds from the prior myopic LASIK. Irregular astigmatism and inferior steepening were skewed and greater OD.
Regarding the clinical management of this patient, I applied in-office microblepharoexfoliation and recommended commercial tea tree oil wipes. These mildly improved his symptoms, yet discomfort from the tea tree oil wipes limited his routine compliance.
At follow-up in December 2023, the patient presented with continued lid itching, redness, and blurry vision that was worse with reading. His BCDVA was 20/60 OD and 20/20 OS, and the clinical examination was unsurprisingly similar to the previous one, with almost diffuse collarettes across both upper eyelids and moderate MGD. I stressed the importance of limiting eye rubbing and prescribed him a new targeted treatment that had been recently FDA approved in the United States. At his next follow-up appointment 11 weeks later, the patient was pleasantly surprised by the significant improvement in itching. He recognized his habit of eye rubbing and stopped himself from reaching up to rub his right eye. I counseled him that the Demodex blepharitis may eventually recur. We also discussed the potential need for repeat CXL if I find evidence of ectasia progression, and I suggested he consider a therapeutic contact lens to optimize his BCDVA.

Treatment
In Europe, we do not yet have an approved, targeted pharmaceutical treatment for Demodex blepharitis. My staff and I follow the standard protocols for our affected patients: education on proper eyelid hygiene, such as rubbing cessation, a cleaning regimen, sleep habits and environment, and discontinuation of any cosmetics. We also ask them to wash their hands before touching their faces, to suppress all possible vectors of infection. For severe blepharitis, we’ll sometimes prescribe an antibiotic for the short term. If we diagnose rosacea, we may prescribe one of the oral cyclines (eg, doxycycline, tetracycline, minocycline) for up to 6 weeks.
Conclusion
Aggressive eye rubbing causes an irregularity of the cornea, and even minor astigmatism. I encourage my colleagues to ask their young patients whether they rub their eyes and look for clinical signs of excessive behavior. Any appearance or worsening of against-the-rule (inverse) or oblique astigmatism in a young patient should prompt ruling out the possibility of early corneal deformation due to excessive eye rubbing. This is when I begin to intervene, informing these patients about the risks of eye rubbing, and I do everything I can to find its cause and improve the health and comfort of the ocular surface.
We’ve now established that Demodex blepharitis can be a major cause of eye rubbing, which puts these patients at higher risk for developing keratoconus. Although the clinical signs look similar to ocular surface diseases, we can easily diagnose Demodex blepharitis at the slit lamp by asking patients to gaze down and looking for collarettes and crusting along the upper lash line. This simple step can help us correctly diagnose Demodex blepharitis in our patients and treat it early to potentially prevent related issues, such as keratoconus, MGD, etc., from developing.
© 2025 Tarsus Pharmaceuticals GL--2500042
1. Fromstein SR, Harthan JS, Patel J, Opitz DL. Demodex blepharitis: clinical perspectives. Clin Optom (Auckl). 2018;10:57-63.
2. Gao Y, Di Pascuale MA, Li W, et al. High prevalence of demodex in eyelashes with cylindrical dandruff. Invest Ophthalmol Vis Sci. 2005;46(9):3089-3094. doi: 10.1167/iovs.05-0275.
3. Rhee MK, Yeu E, Barnett M, et al. Demodex blepharitis: a comprehensive review of the disease, current management, and emerging therapies. Eye Contact Lens. 2023;49(8):311-318.

