
Maps of the corneal epithelium can be valuable in the decision-making process for excimer laser corneal refractive surgery, in the assessment of short- and long-term postoperative outcomes and epithelial healing after corneal collagen crosslinking (CXL), and in screening for keratoconus and pellucid marginal degeneration (PMD). Reinstein et al have contributed a large number of studies with ultrasound epithelial measurements pointing out the plasticity of the epithelium in keratoconic corneas; they have suggested that a thicker than normal central cornea epithelium may suggest ectasia, as it may reflect the thickening normalization response to inferior steepening commonly seen in ectasia.
Current optically based corneal imaging systems have limited capability to discern epithelial from stromal components over the entire corneal area. On the other hand, in vivo visualization of the epithelial layer over the stromal bed can be achieved using the principle of reflecting an elastic wave from the epithelium-stromal interface and detecting its echo.1 Systems employing this technology are known as scanning ultrasound biomicroscopes (UBMs).
We performed a study to explore the efficacy of a highfrequency arc scanning ultrasound system, the Artemis 2+ superior (Arcscan, Inc.) in the task of clinical epithelial corneal mapping in normal and keratoconic eyes. The study included normal eyes, keratoconic eyes treated with the Athens protocol, and keratoconic untreated eyes. The purpose was to examine whether overall increased epithelial thickness can be an indicator for early keratoconus.
Imaging the Epithelium
The corneal epithelium contributes to the refractive power of the cornea, and thus to total ocular refraction. The refractive power of the epithelium alone is an average 1.03 D (range, 0.55–1.85 D) over the central 2.0-mm diameter zone and 0.85 D (range, 0.29–1.60 D) at the 3.6-mm diameter zone.2 Knowledge of the distribution of epithelial thickness may be beneficial in close-call clinical judgments and can aid in screening of candidates for excimer laser corneal refractive surgery. The reason for this is that the epithelium is not of homogeneous depth over the Bowman layer. Often the epithelium compensates for stromal surface irregularities, becoming thicker over valleys and thinner over hills where the stroma protrudes. In other words, the epithelium attempts to minimize abrupt changes in stromal thickness. As a result, the anterior cornea may project a smoother topography and more regular wavefront error map compared with the underlying anterior stroma.
In subclinical corneal ectasia, if the epithelium is thinner over the ectatic area, epithelial profile maps may help a clinician to identify patients in whom corneal ablative procedures are contraindicated.3 Assessment based only on total corneal pachymetry and topography, with no knowledge of epithelial depth, may result in an incorrect assessment of keratoconic progression.
UBM systems
Real-time in vivo epithelial mapping is possible with high-frequency (HF) UBM systems.4-6 The major advantage of ultrasound over optically based systems is that it is not hindered by optically opaque ocular structures.

Figure 1. B-scan reconstruction, as obtained from high-frequency UBM, showing epithelium and corneal thickness measurements via the caliper tool. Anterior and posterior cornea and the cornea-epithelium interface are shown full scan, scale 8.4 μm/pixel (A), and detail (B).
The Artemis digital UBM arc scanner employs a noncontact immersion method7 and is capable of identifying interfaces with localized change in impedance, such as the epithelium to immersion fluid, Bowman interface to anterior stroma, and inferior stroma to aqueous humor. The system achieves resolution of 21 μm, with the precision of measurement varying according to position within the cornea: 0.5 μm at the center and less than 1.3 μm peripherally.8 Examples of B-scan images obtained via the Artemis 2 are presented in Figure 1.
Materials and methods
Our study investigated epithelial characteristics using pachymetric mapping with the Artemis 2+ superior. A total of 33 patients with no clinical finding other than their refractive error, which was biased toward mild myopia, were included in a normal eyes group; of patients diagnosed with keratoconus, 25 were included in an unoperated group and 42 in an Athens–protocol-(AP) operated group. These AP patients received treatment at our facility, and the average elapsed postoperative time was 18.9 ±22.4 months (range, 1 week–6 years).
In some patients, one eye fell into one, while the other into another, category. Of the control group patients, 11 were female and 22 were male; of the 25 unoperated keratoconic patients, 7 were female and 18 were male; and of the 42 AP-treated patients, 13 were female and 29 were male. The bias toward the male population is consistent with our clinical orientation in treating keratoconic patients, and in the fact that keratoconic patients are most likely male.
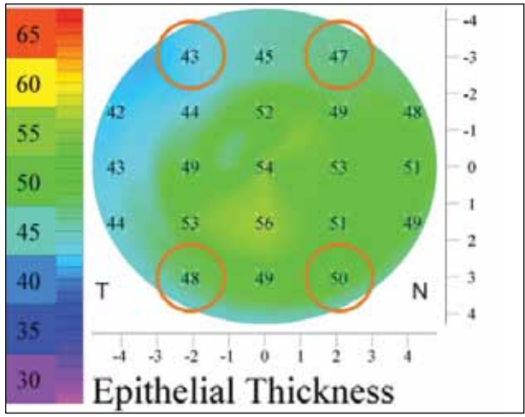
Figure 2. Four transitional zone points were used to calculate peripheral epithelial thickness on each eye. Epithelial thickness from these points was averaged.
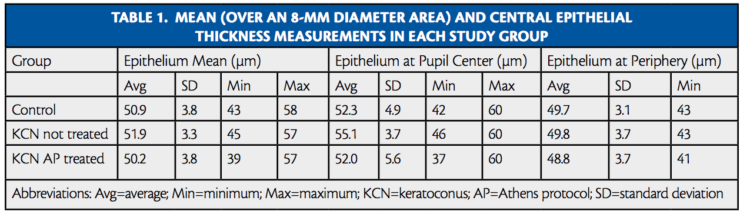
The mean areal epithelial thickness over an area of 8.0- mm diameter and the central epithelial thickness, where the center is defined as the pupil center, were recorded for each eye. We estimated the variation between the center and the periphery for each eye using the average of four points (Figure 2 and Table 1).
Mean, central, and peripheral corneal epithelial thicknesses were compared among the groups. The control group consistently showed thicker epithelium over the pupil center, where the cornea is thinner; however, epithelial thickness varied substantially in the keratoconic groups, both among eyes and within the same eye. In some cases, a difference up to 20 μm between various points on the same eye was observed. Often, the thinner epithelium coincided with the thinner area of the cornea (ie, the cone). However, on average, data from the keratoconic compared with the control group suggested an overall thickening of the epithelium, particularly over the pupil center, on the order of 3 μm. Additionally, the mean epithelial thickness was on average 1.1 μm, and the peripheral transitional zone thickness was almost the same. This thickening was pronounced in the younger patients of the group, suggesting a reactive epithelial response. Eyes treated with the AP showed virtually the same average epithelial thickness (-0.7 μm mean, -0.2 μm over the pupil center, -0.9 over the peripheral zone) as the control group.
DISCUSSION
We observe from the results in Table 1 that our study indicates an average mean corneal epithelial thickness for the normal population of 50.9 ±3.8 μm (range, 43–58 μm), which lies within previously reported values in pertinent publications.10-14
The group of keratoconus patients showed an overall thickening, pronounced at the pupil center. Our results over the whole keratoconus group indicate that, on average, the epithelium at the pupil center was 3.1 μm thicker than the epithelial mean thickness over the entire cornea and that the epithelium at the periphery was on average -2.1 μm thinner compared with the epithelium mean and -5.2 μm compared with the central epithelium.
We believe that the overall thicker epithelium of the keratoconus patients is a result of a reactive process, as the epithelium reacts to the greater susceptibility of the thinner and less rigid cornea to intraocular pressure (IOP) variations. To investigate this hypothesis, we examined separately the five youngest (age, 20.9 ±3.5 years) and the five eldest (age, 33.1 ±3.8 years) patients in the keratoconus group. The results of this analysis indicate that, while the peripheripheral epithelium was identical, the average mean epithelial thickness was by a small margin (0.6 μm) larger in the younger group, and the central epithelium was statistically thicker (2.5 µm) compared with the elder group, indicating that patients in the elder group were more likely to have a smoother epithelium than those in the younger group.
Figure 3. Examples of very smooth epithelium of a patient who underwent treatment with the Athens protocol.
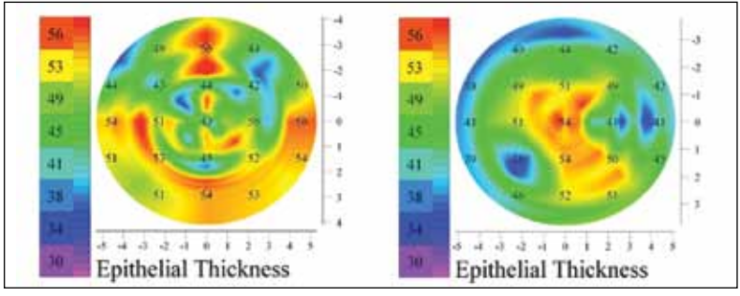
Figure 4. Examples of epithelium of patients who underwent treatment with the Athens protocol demonstrating localized variations.
The AP patients showed epithelial thickness distributions more like the control group, rather than the untreated keratoconic group. In some instances the epithelium was quite normal (Figure 3); however, most often the epithelial map showed local variations (Figure 4).
The clinical impact of these findings may be significant. We have already confirmed these findings clinically with anterior segment optical coherence tomography (OCT; Optovue) in several reports.15-17 Overall epithelial thickness with OCT can be used as a biologic marker of increased corneal oscillation related to ectasia and preectatic states. This information may help clinicians decide, for example, how to treat LASIK regression in a young, highly myopic patient; observation of increased epithelial thickness may guide the clinician toward CXL rather than an additional ablative enhancement. The same principle applies in decision-making for a sibling of a known keratoconus patient who has topographically normal corneas and is being evaluated for a laser refractive procedure.
CONCLUSIONS
Our study demonstrated that epithelial thickness readings, as obtained using arc-scanning HF UBM pachymetry, show substantial localized and between-patient variation. Eyes that did not undergo any surgery showed a moderate central epithelial thickening. Overall thicker epithelium, with large variations, was observed in the keratoconus patients. In many instances, the epithelium was significantly thinner over areas of corneal ectasia. While it can be masked by the uncertainty of the readings, this difference may be particularly helpful in close-call clinical decisions, if the difference is prominent enough, and if differences in the thinner area that coincides with the corneal protrusion are large enough to justify a clinical call. Patients who underwent treatment with the AP, however, did not show a statistically significant trend toward thicker central epithelium. In our study, we noticed and reported for the first time that overall epithelial thickness appears increased in ectatic corneas. We, therefore, suggest that overall average increased epithelial thickness may be a very reliable early biological marker of loss of biomechanical corneal stability. We theorize that increased cornea oscillation in biomechanically unstable corneas may incite a reactive epithelial state of increased thickness, noted in the topographically normal contralateral eye of established keratoconus patients. Our study further supports this theory, as it demonstrated thinner-thannormal overall epithelial thickness in highly irregular keratoconic corneas that had been previously treated with CXL and have been stabilized biomechanically.
Careful examination of epithelial thickness and its distribution may be a tool for overall detection of early keratoconus. Our results indicate that (1) highly irregular epithelium is often an indicator for a thicker and ectatic cornea; (2) the epithelium is thinner over the keratoconic protrusion, often by up to 30 μm; and (3) overall, on average, there is a thicker epithelium in keratoconic and possibly preectasia patients. There are instances when this is clinically significant and may aid in clinical screening. Our subsequent experience in utylizing the much easier anterior segment OCT technology (Optovue) in order to image corneal epithelial maps confirms these findings. In an era were most OCT devices will be able to mimic the Optovue paradigm, epithelial imaging may become an easy, objective tool in the diagnosis of biomechanically unstable corneas and perhaps a multitude of anterior segment disorders such as dry eye, delayed epithelial healing and meibomian gland dysfunction.
Take-Home Message
- Current optically based corneal imaging systems have limited capability to discern epithelial from stromal components over the entire corneal area.
- Knowlede of the distribution of epithelial thickness may be beneficial in close-call clinical judgements.
- Assessment based on total corneal pachymetry and topography with no knowledge of epithelial depth may result in an incorrect assessment of
keratoconic progression. - In this study, normal eyes tended to have a thicker epithelium over the pupil center, but epithelial thickness varied substantially in the keratoconic groups.
- Eyes in the AP group had, on avearge, a similar epithelial thickness to the control group.
A. John Kanellopoulos, MD, is the Director of the LaserVision.gr Eye Institute in Athens, Greece, and is a Clinical Professor of Ophthalmology at New York University School of Medicine. He is also an Associate Chief Medical Editor of CRST Europe. Dr. Kanellopoulos states that he is a consultant to Alcon/WaveLight and Avedro, Inc. He may be reached at tel: +30 21 07 47 27 77; e-mail: ajkmd@mac.com.
Ioannis M. Aslanides, MD, PhD, MBA, FRCOphth, is an Assistant Professor at Weill Cornell Medical Center and Medical Director at Emmetropia Mediterranean Eye Clinic in Greece. Dr. Aslanides states that he has no financial interest in the products or companies mentioned. He may be reached at e-mail: i.aslanides@emmetropia.gr.
George Asimellis, PhD, heads the clinical research department of the laservision.gr institute in Athens, Greece. He states that he has no financial interest in the products or companies mentioned.
Ye SG, Harasiewicz KA, Pavlin CJ, Foster FS. Ultrasonic characterization of normal ocular tissue in the frequency range from 50 MHz to 100 MHz. IEEE Transactions on Ultrasonics, Ferroelectrics and Frequency Control. 1995;42:8-14.
Simon G, Ren Q, Kervick GN, Parel JM. Optics of the corneal epithelium. Refract Corneal Surg. 1993;9(1):42-50.
Reinstein DZ, Archer T, Gobbe M. Stability of LASIK in corneas with forme fruste or suspect keratoconus, where keratoconus was excluded by epithelial thickness mapping. Paper presented at: American Academy of Ophthalmology Annual Meeting; November 9, 2008; Atlanta.
Reinstein DZ, Silverman RH, Coleman DJ. High-frequency ultrasound measurement of the thickness of the corneal epithelium. Refract Corneal Surg. 1993;9(5):385–387.
Reinstein DZ, Silverman RH, Trokel SL, Coleman DJ. Corneal pachymetric topography. Ophthalmology. 1994;101(3):432- 438.
Denoyer A, Ossant F, Arbeille B, et al. Very-high-frequency ultrasound corneal imaging as a new tool for early diagnosis of ocular surface toxicity in rabbits treated with a preserved glaucoma drug. Ophthalmic Res. 2008;40:298-308.
Reinstein DZ, Silverman RH, Coleman DJ. High-frequency ultrasound measurement of the thickness of the corneal epithelium. Refract Corneal Surg. 1993;9:385-387.
Reinstein DZ, Silverman RH, Raevsky T, et al. Arc-scanning very high-frequency digital ultrasound for 3D pachymetric mapping of the corneal epithelium and stroma in laser in situ keratomileusis. J Refract Surg. 2000;16:414-430.
Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman, DJ. Epithelial thickness in the normal cornea: threedimensional display with very high frequency ultrasound. J Refract Surg. 2008;24(6):571-581.
Pérez JG, Méijome JM, Jalbert I, Sweeney DF, Erickson P. Corneal epithelial thinning profile induced by long-term wear of hydrogel lenses. Cornea. 2003;22:304-307.
Wang J, Thomas J, Cox I, Rollins A. Noncontact measurements of central corneal epithelial and flap thickness after laser in situ keratomileusis. Invest Ophthalmol Vis Sci. 2004;45:1812-1816.
Wirbelauer C, Pham DT. Monitoring corneal structures with slit-lamp-adapted optical coherence tomography in laser in situ keratomileusis. J Cataract Refract Surg. 2004;30:1851-1860.
Haque S, Fonn D, Simpson T, Jones L. Corneal and epithelial thickness changes after 4 weeks of overnight corneal refractive therapy lens wear, measured with optical coherence tomography. Eye Contact Lens. 2004;30:189-193.
Møller-Pedersen T, Li HF, Petroll WM, Cavanagh HD, Jester JV. Confocal microscopic characterization of wound repair after photorefractive keratectomy. Invest Ophthalmol Vis Sci. 1998;39:487-501.
Kanellopoulos AJ, Asimellis G. Anterior segment optical coherence tomography – assisted topographic corneal epithelial thickness distribution imaging of a keratoconus patient. Case Rep Ophthalmol. 2013;4:74-78.
Kanellopoulos AJ, Asimellis G. Qualitative and quantitative corneal epithelial thickness distribution in dry eyes in comparison to normal, with anterior-segment Optical Coherence Tomography. Submitted to Am J Ophthalmol. 2013
Kanellopoulos AJ, Asimellis G. In vivo three-dimensional corneal epithelium imaging in normal eyes by anterior segment optical coherence tomography: a clinical reference study. Cornea. 2013 (accepted for publication).