
The concept of office-based surgery (OBS) is neither new nor novel in medicine, having been established as an option for select procedures in dermatology (Moh’s surgery), dentistry, and cosmetic surgery. The next wave of this growing trend may well be in ophthalmology.
Daniel S. Durrie, MD, who serves as Chairman of iOR partners, a company that assists ophthalmologists in establishing and maintaining office-based surgical suites, joined host I. Paul Singh, MD, in an episode of Innovation Journal Club to discuss some of the nuances of OBS in ophthalmology, including what may be the biggest question: Is it safe for patients?
According to Dr. Durrie, the short answer to that question is yes, and he has data to back that assertion. When he joined iOR, Dr. Durrie encouraged his partners to track safety outcomes in all procedures performed in office surgical centers the company is involved with. To date, there are data on over 47,000 unique procedures (Figure), and they demonstrate safety outcomes that are comparable to historical benchmarks from published studies of procedures performed in either ambulatory surgery centers (ASCs) or hospital-based outpatient departments (HOPDs).
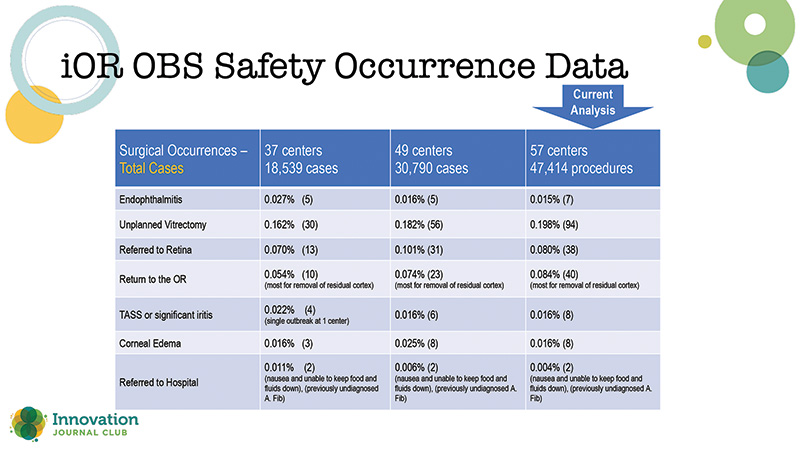
Figure 1. Data on office-based surgery (OBS) performed at centers within the iOR Partners network.
The investigators concluded that, with appropriate protocols, ophthalmic OBS can be performed safely. The analysis is ongoing, and Dr. Durrie expects to amass data on upwards of 70,000 cases by the end of 2024. He has submitted the results of the study for publication in the ophthalmic journals. As he has continued to collect procedure data, he said that the safety rate is staying the same over time.
“It’s safe, as long as you follow a good protocol,” Dr. Durrie said, “as long as you have accreditation standards and do good surgery. We now have three viable safety options, OBS, ASC, and HOPD.“
This is not the first study to show promising safety data on office-based cataract surgery. In 2016, Ianchulev et al published the results of a retrospective consecutive case series of more than 21,000 cataract surgeries that were performed as office-based procedures.1 The investigators found low rates of intra- and postoperative adverse events (and none that threatened vision or life), and they concluded that “Office-based efficacy outcomes were consistently excellent, with a safety profile expected of minimally invasive cataract procedures performed in ASCs and HOPDs.”
Fun and Disruptive
Dr. Durrie recounted to Dr. Singh that he is no stranger to the topic of OBS. In fact, he has been working most of his career to advance the idea, provided it could be proven safe. He was one of the first physicians in the country to offer outpatient cataract surgery in the late 1970s, at a time when patients were typically admitted to the hospital and observed for up to 3 days postoperatively.
“In December of 1979, the hospital was going to kick me off my staff, and my partners were going to kick me out of the office, because I was such a rebel. I thought it was good for patients and stuck with it, and, obviously, outpatient cataract surgery grew.”
Later, when ASCs came of age in the 1980s and 1990s, Dr. Durrie was again on the frontlines, working to form professional societies and encouraging better accreditation standards. Finally, he was at the forefront of the movement to move excimer lasers out of hospitals and ASCs and into dedicated, office-based laser suites so patients could gain easier access to LASIK.
Since those experiences were “fun and disruptive” for Dr. Durrie, he has spent the past decade working toward a wider adoption of OBS for many more types of ophthalmic surgery. Although his safety data are currently dominated by cataract procedures, he said he is seeing growth in office-based glaucoma and retina procedures as well.
What’s in a Name?
The difference between OBS, an ASC, and an HOPD, Dr. Durrie explained, is that OBS falls under the physician’s license or the practice’s license. “It isn’t a separate facility,” he said. Each of these three models has its place in the system of ocular care, Dr. Durrie told Dr. Singh. “[ASCs] are great, as long as you have the volume and the diversity of practice to do that. But [OBS] is more for the smaller practice, or somebody who can’t do an ASC in their state, or somebody who’s putting it in their satellite office.”
Dr. Durrie also sees OBS as a potential answer to the growing disparity between supply and demand in ophthalmology. The rate of cataract procedures is expected to grow over the next 5 years, yet the total number of practicing ophthalmologists is on a downward trend and may decrease by more than 2,500 in that same timeframe. Among the practices in the iOR database, Dr. Durrie said the current volume is ~3,000 ophthalmic procedures per month.
Dr. Durrie said that the results of the safety study have piqued the interest of many ophthalmic colleagues who, with the reassurance that OBS is safe, want to know the details, like how much space they would need to add equipment, the accreditation process, and how reimbursements would work. He described how groups like the Joint Commission and Quad A Global Accreditation Authority have had OBS standards for years, and with the help of iOR and others, now have procedure-specific standards to fit ophthalmology. He added that building an in-office surgical suite is significantly less expensive than building a full ASC, because the latter must be accredited for any type of surgery.
Dr. Singh has incorporated OBS into his practice, and said he feels it gives him a level of control over his surgeries that he doesn’t have elsewhere. He appreciates the continuity of using his staff and equipment, and the ability to control procedure-related costs. And, he told Dr. Durrie: “Our volume of [refractive lens exchanges] and even premium IOLs in the office, bundling it all together, has grown tremendously for us.”
1. Ianchulev T, Liftoff D, Ellinger D, et al. Office-based cataract surgery: population health outcomes study of more than 21,000 cases in the United States. Ophthalmology. 2016;123(4):723-728.

