


Watch the latest episodes of the Innovation Journal Club series on Eyetube.

Can having too many options be bad? When it comes to lens-based options for addressing presbyopia, the answer is “no,” as the array of choices increases the chances of individualizing the selection. Having myriad presbyopia-correcting IOLs available does, however, create some complexity for the clinician when making a recommendation. In episode 9 of Innovation Journal Club, William F. Wiley, MD, offered his take on a recent study of an IOL with extended depth of focus (EDOF) features, and described how he sorts through all the clinically available lens options.
A Novel EDOF Style Lens
A recent study of the xact Mono-EDOF ME4 (Santen Pharmaceuticals)—an IOL with a CE Mark designation as a monofocal that features a biconvex, aspheric design with four diffractive rings—suggested a promising ability to restore far and intermediate vision with low potential for photic phenomena in a small, uncontrolled study.1
In the study, the visual acuity and refractive outcomes at 3 and 6 months were promising (Figure). In reviewing the data, though, Dr. Wiley said what stood out to him was how the investigators focused prominently on the balance between extending depth of focus and minimizing the potential for visual side effects—which is something he sees reflected in the expanding array of IOL options on the market.
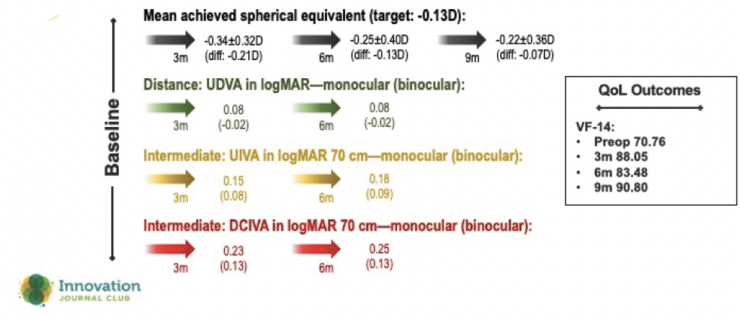
Figure. Three- and 6-month outcomes with a novel EDOF-style lens.
“It seems like there’s a range of different lenses that might give off a little bit more focus, but have a little higher side effect profile, or some that maybe don’t have quite the focus, but have a little lower side effect profile,” he said.
Although the above thinking is an oversimplification of the breadth of options available for patients who want a bit more visual function than what a monofocal can offer, it may provide a framework for presenting options to patients. During consultations, one subtle point Dr. Wiley seeks to understand is the patient’s tolerance for side effects relative to what they want to accomplish with their vision postoperatively.
“Sometimes my decision process is a little bit more binary, where I have full trifocal or full monofocal,” Dr. Wiley said. “The EDOF lenses that sit in between are a little more nuanced to try to tease out … The more we learn about what patients want between the extremes of optimized vision and side effects, we’ll start to find what patient criteria, patient expectations, and personality types fit with those lenses.”
An Ever-Growing Market
Throughout their conversation, Drs. Wiley and Singh addressed a question many surgeons face on a daily basis: How, exactly, do you sort through the options so that patients are offered the best lens for their individual optical system—and what criteria or patient factors are most helpful in making that determination?
In his clinic, Dr. Wiley said he takes a decidedly conservative approach to IOL selection, looking for reasons on the physical exam and imaging that would exclude a patient from a multifocal. Sometimes the best use of surgical judgment is deciding when not to offer certain options.
“What might be ‘premium’ for a particular optical system may be excluding a complex optical system. Some eyes may not be able to handle a complex optical system, and if you try to add that in with a multifocal, you could be making the optical system more complicated,” Dr. Wiley said.
However, he added that he may have to revisit how he uses so-called “premium lenses” as options that are more suitable for complicated cases that come to the clinic. For example, early experiences with the IC-8 (AcuFocus), which features small-aperture optics, suggest it may be viable for aberrated corneas, eyes that are post-refractive surgery, and in eyes with mild retinal pathology—cases for which traditional multifocals are considered less than ideal.
“What we find is that aperture optics take great intermediate vision and extend the focus both ways, extending both distance and near vision,” Dr. Wiley said. “We’re so used to thinking about presbyopia correction as [an addition]—you take plano and add something to it just in one direction, but aperture optics extends focus on both sides of that curve.”
Aperture optics might also be an option for patients who are considering monovision. Although pseudophakic monovision can be successful in many cases, hitting the refractive target is crucial, as any refractive surprise tends to get magnified. The pinhole effect from the IC-8, which is more forgiving in this regard, may be a consideration, especially if the patient did not have success with monovision contact lenses.
In a similar fashion, the Light Adjustable Lens (RxSight) could be an answer for patients who are uncertain whether monovision is right for them. Because the surgeon can titrate the lens power postoperatively, patients can be targeted for monovision initially, for example, and then do a real-world trial to see if their new vision is suitable for their lifestyle.
“We’ve had a lot of success with the Light Adjustable Lens,” Dr. Wiley said. “It has some spherical aberration that’s built into the system, so we do see some depth of focus gains that rival other lenses as far as the range of vision. Plus, it’s very precise on hitting those targets—we know we can nail that distance vision and nail that monovision target if that’s what the patient wants.”
1. Baur ID, Khoramnia R, Weindler J, et al. Clinical outcomes of a new hybrid monofocal iol with extended depth of focus. J Refract Surg. 2021;37(9):601-608.