
Introduction
Posterior capsule rupture (PCR) is common and one of the most consequential complications of cataract surgery.1 Traditional phacoemulsification tips have a metal cutting edge at the aspirating distal end.2 Ruptures most frequently occur during the phacoemulsification stage of the cataract surgery procedure due to unintended contact of the phacoemulsification tip with the posterior capsule.3 Posterior capsule rupture might be associated with vitreous loss, higher rates of endophthalmitis, and retinal detachment.3,4 Uneventful cases had significantly better visual outcomes than ones complicated with PCR.5

Figure 1. ACTIVE SENTRY® Handpiece with INTREPID® Hybrid Tip
The INTREPID® Hybrid Tip is an innovative phacoemulsification tip with a high-strength polymer coating on the distal end. The Hybrid Tip has the same overall design and dimension as the INTREPID® Balanced Tip and is still composed of metals, although the distal end has an overlying polymer coating.2,6,7 The Hybrid tip is designed to minimize damage to the capsular bag and other tissues.7,8 The INTREPID® Hybrid Tip is a polymer-ended phacoemulsification tip for use with the Active Sentry® handpiece (Figure 1).9 The Active Sentry® technology allows faster mitigation of surge response ensuring anterior chamber stability (Figure 2).10-13 The INTREPID® Hybrid Tip synergistically with Active Sentry® technology may improve surgical comfort and confidence by lowering the risk of damaging the ocular tissues.8,10-13
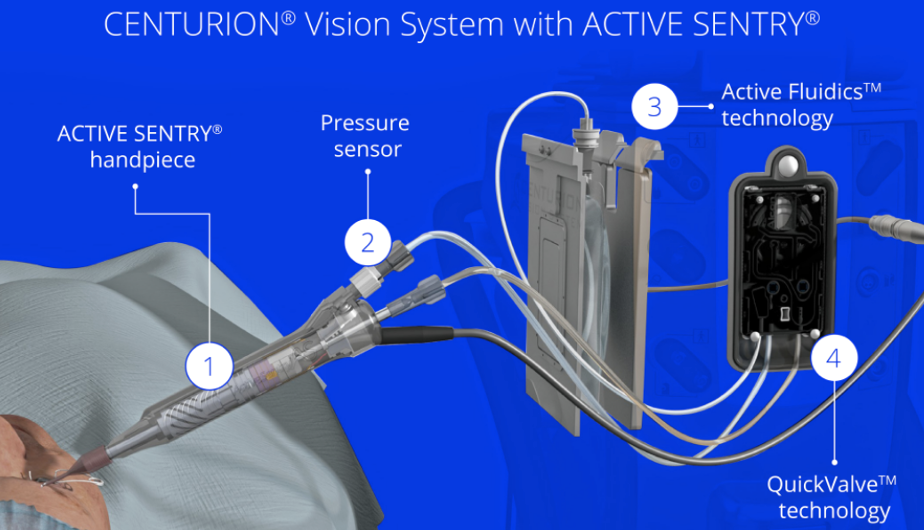
Figure 2. 1. Active Sentry® Handpiece: Signals to CENTURION® hardware and software that adjustments are needed to maintain consistent IOP. 2. Pressure Sensor: Detects changes in anterior chamber stability as they occur. 3. Active Fluidics™ technology: Uses compression plates to adjust the pressure on the BSS irrigating solution bag, compensating for changes in the eye. 4. QuickValve™ technology: Releases fluid into the aspiration line and minimizes occlusion break
INTREPID® Hybrid Tip laboratory performance
The INTREPID® Hybrid Tip was tested in several experimental studies. Shumway et al. evaluated the capsular safety of a new hybrid phacoemulsification tip in a cadaver eye model. Two phacoemulsification tips INTREPID® Hybrid Tip (hybrid tip) and INTREPID® Balanced Tip (metal tip) were tested using 10 phakic cadaver eyes. After lensectomy, the posterior capsule was subjected to direct contact with the tested tip. The vacuum limit was set to 150 mmHg, and the aspiration flow rate to 30 cc/min then torsional power increased in 5% increments up to a maximum of 60%. The primary endpoint was the torsional power required to produce a PCR. The results showed that the hybrid tip required significantly higher torsional power to produce a PCR than the metal tip indicating a lower likelihood of PCR with the INTREPID® Hybrid tip (Figure 3).7

Figure 3. Mean torsional power required for posterior capsule rupture with bevel tip positioned upward.
Another experimental study used porcine eyes to compare INTREPID® Hybrid Tip (Hybrid tip) vs INTREPID® Balanced Tip (Metal tip) by the risk of capsule rupture under the different conditions of longitudinal, torsional, and a combination of ultrasound power modes. After making a corneal incision, the phacoemulsification tip was pressed against the anterior capsule. The IOP was set to 20 mmHg and the aspiration flow rate to 30 cc/min. Under the two aspiration powers of 0 and 200 mmHg, the ultrasound power was set to 5% and increased in increments of 5% with a change in the position on the anterior capsule pressed by the tip. These steps were repeated using longitudinal, torsional, and combination modes. The mean ultrasound power among increments one step before rupture was determined as the maximum value that did not cause rupture (threshold). One hundred twenty porcine eyes were used for the experiments (10 eyes for each condition). The Metal tip showed capsule rupture with a smaller ultrasound power than the Hybrid tip, regardless of power mode or aspiration power. The torsional mode in the Hybrid tip group showed the highest ultrasound power causing capsule rupture compared to all other groups (Figure 4).14

Figure 4. Ultrasound power (%) threshold to cause capsule rupture. *P value <.001, Kruskal-Wallis followed by Scheffe’s post hoc test
Zacharias2 compared the in vitro incisional temperature, acoustic energy, transient cavitation, and turbulence of the Hybrid Tip and Balanced Tip. Both tips were used with Active Sentry® handpiece in a torsional mode. Mini-flared Kelman tip was used as a control for the thermal profile testing only. Controlled loads were applied over the tip sleeve simulating the pressure at the corneal incision. Generated heat was recorded on a blackbody filmstrip using infrared imaging, and 360° mapping of acoustic pressure was registered using a directional hydrophone. Cavitation patterns with increasing ultrasound power were imaged with high-speed video recording and particle image velocimetry was used to evaluate turbulence, streaming, and bubble formation. The study showed the following results: the temperature rise for the Hybrid and Balanced tips was lower than with the control mini-flared Kelman tip (P≤0.0001). The Hybrid tip generated reduced acoustic output compared with the Balanced tip; the ultrasound threshold for cavitation was higher for the Hybrid versus Balanced tip (55% vs 25%) and fluid turbulence was more evident with the Balanced tip compared with the Hybrid tip.2
Cardenas et al.15 performed an experimental study in porcine lens cubes to compare the efficiency of the Hybrid Tip with the Balanced (metal) Tip. Efficiency was assessed using cumulative dissipated energy (CDE) and total procedure time. The lens was removed from the eyes and the capsule then was placed in formalin solution to achieve a density similar to grade 4+ cataracts in humans. The hardened lenses were washed with a balanced salt solution (BSS) and cut into uniform, 2 mm cubes. The prepared lens cubes were placed into an artificial anterior chamber filled with BSS, and experimentation was performed on the same day to prevent further lens hardening or tissue degradation. Phacoemulsification was performed using Hybrid Tip or Balanced Tip. The vacuum was set at 500 mmHg and the aspiration flow rate at 50 mL/min. Power was changed for torsional and longitudinal ultrasound at 20%, 40%, 60%, 80%, and 100%. Two hundred porcine lens cubes were used, 10 for each specified tip/power setting. Study results indicated comparable CDE and procedure times between the two tips at all power levels and ultrasound modes. Longitudinal ultrasound showed decreased efficiency as power increased, attributed to increased lens fragmentation (chatter). Torsional ultrasound, on the other hand, demonstrated increased efficiency up to 60% power, with no significant differences beyond that threshold (Table 1).15

The number of publications providing data on Hybrid Tip clinical performance is limited. The results of one retrospective study8 were published. The study compared the efficacy and safety of cataract procedures performed using Centurion with Active Sentry® handpiece with INTREPID® Hybrid tip (n=86 eyes) and Centurion with Ozil handpiece with INTREPID® Balanced tip (n=82 eyes). The investigators reported that CDE in the Hybrid tip group was significantly lower than in the Balanced tip group (8.8 ±3.9 and 10.4±4.2, p-value 0.016), the torsional amplitude was also significantly lower in the Hybrid tip group (51.2 ±13.3 and 65.2±9.3, p-value 0.000). No differences in total ultrasound time were detected. Posterior capsule rupture (2 eyes) and iris damage (1 eye) were reported in the Balanced tip group and no complications in the Hybrid tip group.8 The authors of the published laboratory and clinical studies highlighted that the Hybrid tip would be useful for experienced surgeons as well as for those who are in training.7,8,15 Further studies are needed to evaluate the Hybrid tip in clinical settings.
Conclusions
INTREPID® Hybrid Tip is a polymer-ended phacoemulsification tip. The Hybrid Tip significantly decreased the risk of capsule rupture in a laboratory setting.7,14 The Hybrid Tip had lower acoustic output, lower cavitation, and lower turbulence compared with the metal tip, suggesting the potential for improved clinical safety.2. The Hybrid Tip showed comparable efficiency with the metal tip in an experimental and clinical environment.8,15
The views and opinions expressed here do not necessarily represent those of Bryn Mawr Communications or Cataract & Refractive Surgery Today Global.
© 2024 Alcon Inc. 10/24 IMG-CNT-2400041
1. Liu YC, Wilkins M, Kim T, Malyugin B, Mehta JS. Cataracts. Lancet 2017; 390:600–612
2. Zacharias J. In vitro analysis of clinically relevant aspects of a polymer-coated phacoemulsification tip vs a traditional tip. J Cataract Refract Surg 2023; 49:1264–1269
3. Zare M, Javadi MA, Einollahi B, Baradaran-Rafii AR, Feizi S, Kiavash V. Risk factors for posterior capsule rupture and vitreous loss during phacoemulsification. J Ophthalmic Vis Res 2009 Oct;4(4):208-12
4. Yap EY, Heng WJ. Visual outcome and complications after posterior capsule rupture during phacoemulsification surgery. Int Ophthalmol 1999; 23:57–60
5. Ti SE, Yang YN, Lang SS, Chee SP. A 5-year audit of cataract surgery outcomes after posterior capsule rupture and risk factors affecting visual acuity. Am J Ophthalmol 2014; 157:180–185.e1
6. Centurion® Vision System FMS Pack Directions for Use
7. Shumway C, Ellis N, Heczko J, Jiang B, Werner L, Mamalis N. Evaluation of the capsular safety of a new hybrid phacoemulsification tip in a cadaver eye model. J Cataract Refract Surg 2019; 45:1660-1664
8. Sabur H., Unsal U. The efficacy and safety profile of cataract procedures performed with a sensorembedded handpiece and a new hybrid phaco tip Eur J Ophth 2022 Nov;32(6):3438-3443
9. Centurion® Vision System Operator’s Manual
10. Miller KM, Dyk DW, Yalamanchili S. Experimental Study of Occlusion Break Surge Volume In 3 Different Phacoemulsification Systems. J Cataract Refract Surg. 2021;47:1466-1472
11. Suzuki H., Igarashi T, Takahashi H. Effect of a new phacoemulsification and aspiration handpiece on anterior chamber stability. J Cataract Refract Surg 2023; 49:91–96
12. Thorne, A., Dyk, D. W., Fanney, D. & Miller, K. M. Phacoemulsifier occlusion break surge volume reduction. J Cataract Refract Surg 2018; 44, 1491-1496
13. Vasavada V, Vasavada AR, Vasavada VA, Vasavada SA, Bhojwani D. Real-Time Dynamic Changes in Intraocular Pressure After Occlusion Break: Comparing 2 Phacoemulsification Systems. J Cataract Refract Surg. 2021;47:1205-1209
14. Ichikawa Kei, Tanaka Y, Tokiwa S, Naito A, Hidaka Y, Reiko Ichikawa R, Ichikawa Kazuo. Comparison of INTREPID® balanced and hybrid tips on anterior capsule rupture in ex vivo porcine eyes. PLOS ONE August 29, 2023 https://doi.org/10.1371/journal.pone.0290657
15. Cardenas IA, Ungricht EL, Zaugg B, Olson RJ, Pettey JH. Efficiency of a polymer-coated phacoemulsification tip in cataract surgery. J Cataract Refract Surg. 2023 Oct 1;49(10):1056-1060.
Please refer to relevant product’s instructions for use for complete list of indications, contraindications and warnings.
Market-specific safety information may be required. The product(s) may not be available in your market. Please check the availability with your local representative.



