


KEY TAKEAWAYS
- Posterior capsular rupture shifts the priority from phacoemulsification to chamber stabilization, vitreous clearance, and preservation of the anterior capsulorhexis
- Diagonal haptic capture uses a centered continuous capsulorhexis and four-haptic acrylic IOL to cross-lock the lens without sulcus contact or sutures
- Diagonal haptic capture provides a fast, atraumatic rescue strategy with durable IOL centration when the anterior capsulorhexis remains intact
A 60-year-old patient presented with a progressive decline in visual acuity due to a visually significant cataract. A preoperative slit-lamp examination showed 2+ nuclear sclerosis with no evidence of zonular weakness. Biometry and corneal measurements were unremarkable, and the patient consented to standard phacoemulsification with implantation of an aspheric IOL.
Even in eyes with no preoperative red flags, posterior capsular rupture (PCR) remains an intraoperative risk. In my clinical experience, the key determinant for long-term stable IOL fixation and a great visual outcome appeared to be not the complication itself but the speed and amount of trauma induced by the fixation strategy once capsular support was compromised.
This article briefly presents the technique of diagonal haptic capture (DHC)1 and its benefits, as described in a retrospective series of 20 eyes evaluating DHC with up to 10 years of follow-up.2
INTRAOPERATIVE COURSE AND RECOGNITION OF THE COMPLICATION
In the case example provided earlier, phacoemulsification proceeded routinely through creation of the capsulorhexis, hydrodissection, and nuclear disassembly. During removal of the final nuclear fragment, however, a sudden increase in anterior chamber depth and a subtle loss of followability signaled a PCR.
At that point, my goals were straightforward: stabilize the chamber, relieve vitreous traction, and preserve the anterior capsular rim because that structure ultimately determines the options for IOL fixation.
CHAMBER STABILIZATION AND VITREOUS MANAGEMENT
Phacoemulsification was halted immediately, and a dispersive OVD was injected through the paracentesis to tamponade the rupture and prevent further vitreous migration. The instruments were withdrawn only after the anterior chamber had fully stabilized.
A bimanual anterior vitrectomy was then performed with a high cut rate and a low aspiration flow rate to minimize vitreoretinal traction. Diluted triamcinolone (1:5) was injected to confirm complete vitreous clearance from the anterior chamber and wounds. Importantly, no attempt was made to chase lens material that might have descended posteriorly because doing so could have enlarged the capsular defect. The remaining cortex was removed carefully.
ASSESSING CAPSULAR SUPPORT: THE DECISION POINT
Once the anterior chamber was quiet and stable, my attention turned to IOL fixation. The posterior capsule had clearly ruptured, but the anterior capsulorhexis remained intact, continuous, and well centered. The latter finding has fundamentally changed my management strategy in this situation since 2015.
Traditional options in this setting include sulcus placement of a three-piece IOL, scleral fixation, and iris fixation. Each carries short- and long-term risks, including lens tilt and decentration, uveal irritation, secondary glaucoma, cystoid macular edema, suture-related complications, and refractive unpredictability.
DHC TECHNIQUE
The originally planned four-haptic hydrophilic acrylic IOL (Akreos Adapt AO, Bausch + Lomb) was implanted because its haptics are well suited to DHC. Two diagonally opposed haptics were positioned posterior to the anterior capsulorhexis, and the remaining two haptics were gently captured anterior to the capsular rim in a diagonal configuration. This created a stable cross-locking effect that distributed forces evenly across the capsular opening (Figure 1).
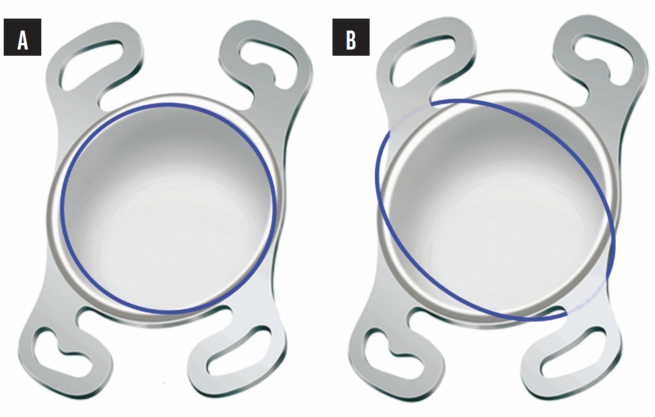
Figure 1. Normal haptic positioning (A). DHC schematic showing alternating haptic positions relative to the anterior capsulorhexis (B).
Key technical points include the following:
- The capsulorhexis must be continuous, curvilinear, and well centered; and
- Stress on the anterior capsule and zonules is reduced by minimizing manipulation.
Unlike classic optic capture, DHC provides secure fixation without sulcus contact or scleral suturing while maintaining excellent IOL centration and minimizing uveal contact.
POSTOPERATIVE COURSE AND OUTCOME
On postoperative day 1, the cornea showed mild edema, as expected, and the anterior chamber was quiet. The IOL was well centered, IOP was within normal limits, and no vitreous was evident in the anterior chamber.
Ten years after surgery (Figure 2), the patient’s BCVA was 1.0, and the refraction was stable. There was no evidence of pigment dispersion, chronic inflammation, or IOL tilt. These findings were consistent with the long-term outcomes observed in the retrospective series mentioned earlier, which found sustained IOL stability, favorable refractive results, and a low incidence of uveal complications after DHC.
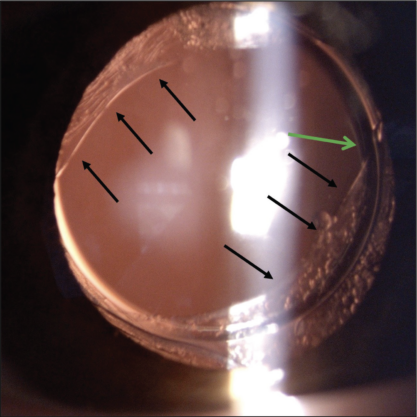
Figure 2. Postoperative slit-lamp photograph demonstrating excellent IOL centration and stability. Black arrows indicate the ovalized capsulorhexis; green arrows indicate a haptic positioned anterior to the capsulorhexis.
WHY DHC HAS BECOME MY PREFERRED RESCUE STRATEGY
DHC has become one of my strategies for managing complications for several reasons. First, it allows me to use my preferred routine IOL (whether a spherical or aspheric model) without changing its power. Second, DHC leverages the patient’s current ocular anatomy—an intact anterior capsulorhexis—instead of bypassing it. Third, DHC avoids complications related to sutures and/or the iris. Fourth, the technique appears to provide long-term IOL stability. Finally, DHC is reproducible, atraumatic, and efficient, even in the setting of an intraoperative complication.
TAKE-HOME MESSAGE
A ruptured posterior capsule does not have to compromise the surgical outcome. When the anterior capsule is preserved, DHC of a four-haptic acrylic IOL can provide a minimally traumatic, stable, and durable solution that bridges the gap between IOL implantation in the bag and more invasive secondary fixation techniques.
In the case example presented in this article, the patient’s outcome has remained excellent through 10 years of follow-up. In my broader experience with this specific IOL, outcomes have been excellent, but results could differ with other lens designs.
1. Jin H, Zhang H. Diagonal haptic capture of a plate intraocular lens with 4 haptics. J Cataract Refract Surg. 2020;46(4):503-506.
2. Taneri S, Förster T, Grigat M, Dick HB. Diagonal haptic capture of an acrylic intraocular lens: long-term safety and efficacy. J Cataract Refract Surg. In press.
