
To capitalize on the greater strength and uniformity of a capsulotomy edge created with a femtosecond cataract laser, Teleon Surgical developed the FEMTIS® family of IOLs as the perfect lenticular complement: a premium platform providing monofocal, multifocal, and extended depth-of-focus (EDOF) options that fixates to the anterior capsulotomy to maximize stability and minimize visual phenomena. The FEMTIS IOL Family includes three models: the monofocal FEMTIS, the FEMTIS Comfort MF15 (EDF), and the FEMTIS Mplus MF 30 (FVR). The latter two models each include a toric option for astigmatic correction.
I now have been implanting the FEMTIS family of IOLs for 10 years, and I continue to recommend these lenses to my patients. This article provides an overview of the lenses and results from a multicenter, multinational study of the FEMTIS Comfort MF15 IOL, and it details my personal 5-year experience implanting this lens.
FEMTIS IOL Design
All the FEMTIS IOLs are constructed in a plate-haptic design with additional clip-style haptics (two large, longitudinal haptics, and two small, latitudinal haptics) to form a secure unit with the rim of the capsulotomy. This design minimizes common complications of premium IOLs such as instability and tilt, decentration/rotation, refractive predictability errors, and dysphotopsias as well as other visual phenomena (Figure 1).

Figure 1. Although the capsulorhexis margin of a standard, bag-fixated IOL has the potential to cause symptoms of negative dysphotopsias (left), the rim of the FEMTIS IOL forms an ideal unit with the rim of the capsulotomy, thereby preventing dysphotopsias (right).
The FEMTIS IOL’s total diameter is 10.5 mm, with an optic size of 5.7 mm. The optic is an aspheric, biconvex, aberration-neutral design composed of the company’s proprietary Hydrosmart® material, which is a copolymer of hydrophilic acrylates that contain 25% water. Its surface has hydrophobic properties that absorb UV light , and the entire FEMTIS family offers naturalistic color perception.
FEMTIS Comfort MF15
The FEMTIS Comfort MF15 IOL is designed for patients who want to prioritize excellent distance and intermediate vision in daily life with a 1.50 D add. This lens offers extended depth of focus (EDOF) with an uninterrupted distribution of light through the optic segments—what the company refers to as a varifocal effect. The central optical zone reduces recipients’ sensitivity to potential IOL decentration and tilt because the distance visual acuity is not influenced by minor decentration (Figure 2). All patients who desire increased spectacle independence and who have no problems with occasionally wearing reading adds are perfect candidates for this IOL. Also, patients who frequently drive at night will benefit from its very low scotopic phenomena.
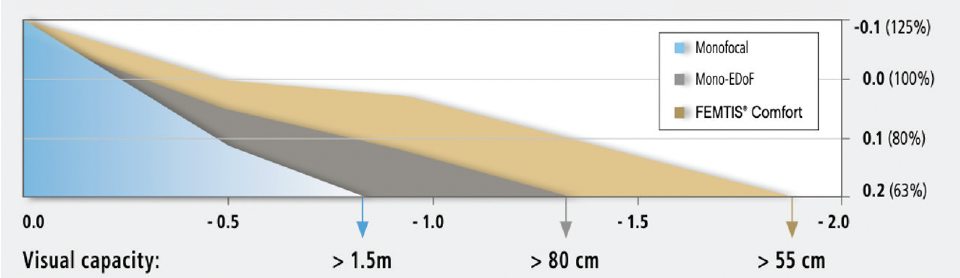
Figure 2. Comparison of defocus capacity of the FEMTIS Comfort IOL, a monofocal IOL, and a monofocal plus IOL.
The FEMTIS Comfort Toric MF15T IOL offers all the benefits of the Comfort optic, but with additional astigmatic correction of +0.75 D, +1.50 D, +2.25 D, and +3.00 D. Its aberration-neutral optic provides excellent contrast sensitivity and depth of focus for low lighting conditions. Because this lens fixates to the anterior capsulorhexis, it can be rotated in either direction before being enclaved to the edge.1
The FEMTIS MPlus MF30
The FEMTIS Mplus and Mplus Toric IOLs (FB-313 MF30T) are multifocal options to correct presbyopia and astigmatism. This model has 3.00 D of near addition and a large aspheric distance optical zone that maximizes light transmission for sharp distance vision with excellent contrast sensitivity. Yet, its Continuous Transmission Technology and its segmented varifocal optical zones that are spread across the prolate surface enable a smooth transition between distance and near viewing, with minimal photopic phenomena. Because this IOL offers a full range of vision, it is ideal for patients who demand complete spectacle independence.
NO ANTERIOR CAPSULAR FIBROSIS WITH FEMTIS IOLS
What I especially love about the FEMTIS lenses is checking my patients’ eyes after implantation and seeing absolutely no part of the anterior capsule in front of the optic. This results in very good optical performance, especially in mesopic conditions and wide pupils. Because of their design, FEMTIS IOLs keep the anterior capsule remarkably free of fibrosis. With standard IOLs, I often find fibrosis a few years after implantation, but not so with the FEMTIS IOLs (Figure 3).

Figure 3. Two years after implantation, an eye with a FEMTIS IOL shows no signs of anterior capsular fibrosis (left), compared to an eye that received a standard in-the-bag monofocal IOL (right).
The learning curve for implanting the FEMTIS IOLs is very short. It can be implanted under viscoelastic or simple irrigation (there is an advantage to not having to remove viscoelastic from behind the IOL). The only instrumentation needed is a small hook for assisting with the enclavation of the lens, such as a Sinskey hook. The enclavation maneuver is very quick, in my experience.
Results of a Yearlong Multicenter Study
I participated in a yearlong, multinational case series that encompassed eight study sites across Germany, Spain, Great Britain, and Andorra to determine the stability of the effective lens position of the monofocal FEMTIS Comfort IOL up to 1 year after implantation following femtosecond laser-assisted cataract surgery with the LENSAR laser.2 Colleagues and I enrolled a total of 183 patients (366 eyes) with senile cataracts. The study’s main endpoints were IOL decentration, rotation, and tilt (horizontal and vertical) compared to published data on standard IOLs. Secondary endpoints were the distance between the iris and the IOL’s final resting place, and patients’ subjective refraction, UCVA, and incidence of posterior capsular opacification (PCO). We performed FLACS in each eye, and then we implanted IOL powers of 15.00 to 27.00 D. We targeted postoperative astigmatism for <1.00 D. The patients were evaluated preoperatively and then at days 1-7, weeks 6-8, and at 6 and 12 months after surgery.
Centration
The centration of the FEMTIS Comfort IOL over 12 months was excellent (Figure 4).
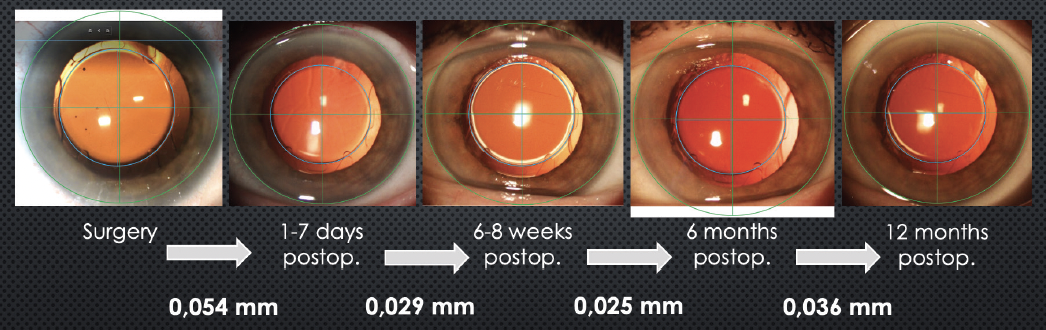
Figure 4. In an international, multicenter study of the FEMTIS Comfort MF15 IOL, the lens’ effective lens position was remarkably stable over 12 months.
Compared to published studies of capsular-bag-implanted IOLs, the FEMTIS Comfort showed very high rotational stability over 12 months. Whereas some published studies recorded up to 5º of IOL rotation within 6 months of implantation, the FEMTIS Comfort IOL showed no more than 0.78º of rotation out to 12 months.
Decentration of the FEMTIS Comfort lens was also excellent, compared with published results of standard bag-implanted IOLs. Its mean decentration from postoperative day 1 to 6 weeks was 0.07º; from 6 weeks to 6 months, the lens’ mean decentration was 0.08º; and from 6 months to 12 months, the mean was 0.07º. These averages were compared against the published results of three studies, which recorded mean IOL decentration between 6 weeks and 6 months postoperatively as 0.57º, 0.42º, and 0.38º.3-5
Tilt
In our multicenter study, the FEMTIS Comfort IOL showed a minimal degree of horizontal and vertical tilt. The lens showed a mean horizontal tilt of 0.79º from preoperative measurements to 6 weeks after implantation (compared to a mean of 2.50º in three published studies); 0.49º of horizontal tilt from 6 weeks to 6 months; and 0.48º of tilt from 6 to 12 months. Mean vertical tilt for the FEMTIS Comfort lens was 1.29º, 1.08º, and 1.37º over the same timeframes.
Surgeon Questionnaire
Finally, we surgeons in the study filled out a questionnaire about our experience implanting the FEMTIS IOL. Here, the FEMTIS received high marks for injection into the eye, the ease of removing viscoelastic from behind the lens, and positioning the large haptics in front of the capsulorhexis. The positioning of the two smaller haptics in front of the capsulorhexis required slightly more maneuvering but was still deemed “easy” (Figure 5).

Figure 5. In the FEMTIS multicenter study, surgeons gave high marks to their experience implanting the FEMTIS IOL. (Data adapted from Auffarth GU, et al. Stability and visual outcomes of the capsulotomy-fixated Femtis-IOL after automated femtosecond laser-assisted anterior capsulotomy. Am J Ophthalmol. 2021.)
Visual Acuity
Patients’ visual acuity outcomes remained strong throughout 12 months. Mean distance-corrected visual acuity (DCVA) reached 0.00 ± 0.08 logMAR by 6 months, and -0.01 ± 0.09 logMAR at 12 months. By 12 months postoperatively, 97.5% of the study eyes had achieved 0.1 logMAR DCVA, likely due to the stability of the IOL’s centration.
TAKEAWAYS
The FEMTIS Comfort MF15 IOL provides effective uncorrected intermediate and distance visual acuity that is comparable with other EDOF IOLs. It has an excellent defocus curve and gives patients strong visual acuity and contrast sensitivity in mesopic conditions. In 5 years of follow-up with my cohort from the 12-month multicenter study (unpublished data), I’ve seen safe, stable results, and no intra- or postoperative complications. Compared to published results with standard IOLs, the FEMTIS shows better stability and refractive predictability. I attribute this functional performance to the combined benefits of the FLACS technique with a capsulotomy-fixated EDOF lens.
1. Data on file: Clinical evaluation of the rotational stability, Prof. B. Dick, University Hospital Bochum.
2. Auffarth GU, Friedmann E, Breyer D, et al. Stability and visual outcomes of the capsulotomy-fixated femtis-iol after automated femtosecond laser-assisted anterior capsulotomy. Am J Ophthalmol. 2021;225:27-37.
3. Lee D-H, Shin S-C, Joo C-K.Effect of a capsular tension ring on intraocular lens decentration and tilting after cataract surgery. J Cataract Refract Surg. 2002; 28(5):843-6.
4. Findl O, Hirnschall N, Wiesinger J. Effect of manual capsulorhexis size and position on intraocular lens tilt, centration, and axial position. J Cataract Refract Surg. 2017; 43(7):902-908.
5. Mester U, Sauer T, Kaymak H. Decentration and tilt of a single-piece aspheric intraocular lens compared with the lens position in young phakic eyes. J Cataract Refract Surg. 2009;35(3):485-90.

