
Sponsored By

Experience With PRESBYOND as a Surgeon-Patient
Most refractive surgeons know about the variety of available procedures to help patients cope with presbyopia, and some have even themselves undergone procedures that aim to compensate for presbyopia. One of these surgeons is Sri Ganesh, MBBS, MS, DNB, of the Nethradahama Super Specialty Eye Hospital in Bangalore, India, who underwent PRESBYOND Laser Blended Vision in November 2015.
By age 45, Dr. Ganesh had difficulty reading small print in dim light, and he noticed problems with intermediate vision by age 47. He recognized that he could try multifocal contact lenses, but he wanted a solution that would provide him with more function and more freedom. In addition to PRESBYOND, Dr. Ganesh considered corneal inlays, monofocal and multifocal LASIK, refractive lens exchange, and a presbyopic phakic IOL. He selected PRESBYOND because of the procedure’s high rate of patient satisfaction; the good functional vision, contrast sensitivity, and stereopsis it provides; and the facts that there is no permanent visual effects (glare and halos) and that the procedure is reversible.
The procedure was performed by Dan Z. Reinstein, MD, MA(Cantab), FRCSC, DABO, FRCOphth, FEBO, of the London Vision Clinic. Preoperatively, Dr. Ganesh’s refraction was +1.00 +0.50 X 170º in his right eye and +1.00 +0.50 X 180º in his left. At 1-year postoperative, Dr. Ganesh’s sphere improved to 0.25 D in his right eye and -1.75 D in his left. His binocular UCVA was 6/3. He said that he is very satisfied with his vision and would strongly recommend the procedure to his colleagues as well as to his patients.
A Refractive Surgeon’s Refractive Surgery
As a lifelong myope, Robert Morris, MRCP FRCS, FRCOphth, of Grange Eye Consultants, United Kingdom, was used to dealing with contact lenses and spectacles. However, by age 61, he had become contact lens intolerant, and monovision was no longer an effective approach to managing his presbyopia. Further, he could no longer wear his glasses at the microscope and the slit lamp. Although Dr. Morris had blepharitis, superficial keratitis, few guttata, and mild age-related lens changes, his OCT findings were normal and the refraction in his right and left eyes (-4.00 -1.25 X 79º and -5.25 -0.25 X 74º, respectively) were well within the range of a variety of procedures.
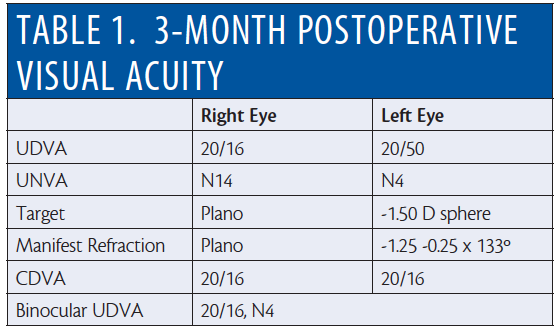
Dr. Morris decided to undergo PRESBYOND Laser Blended Vision with the VisuMax femtosecond laser (ZEISS). Dr. Reinstein performed the procedure in February 2017. On day 1 postoperative, Dr. Morris had achieved a CDVA of 20/16 in both eyes, and this was maintained through 3 months postoperative (Table 1). AcuTarget HD (AcuFocus) depict the ocular scatter and objective refraction images at 3 months postoperative (Figure 1).
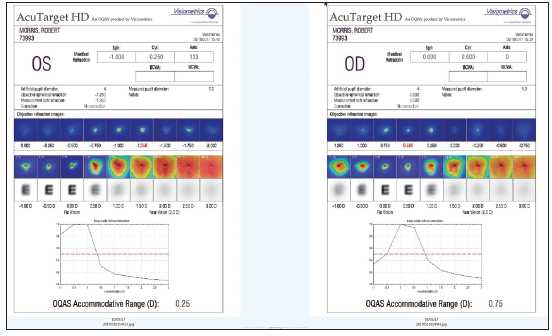
Figure 1. Ocular scatter index imaging of Dr. Morris’ eyes at 3 months postoperative.
Dr. Morris said that, after PRESBYOND, his binocular distance vision is the best it has ever been. He is spectacle independent, minus needing readers in poor-light conditions when he is tired. Although he experienced some dry eye for the first month postoperative, his dry eye symptoms have improved and he no longer requires eye drops.
SMILE: Tips and Tricks for Managing Different Situations
Also discussed at the 2017 ZEISS European Refractive Laser Symposium in Paris was how to manage complications after small incision lenticule extraction, or SMILE.
A Case of Late Lenticule Extraction
Speaking about solving lenticule extraction issues, Marco Fantozzi, MD, of the Camaiore Hospital, Lucca, Italy, shared a case of late lenticule extraction. In this case, during the initial procedure, the lenticule was dissected in only the lower plane, instead of in the upper plane first, by a fellow surgeon. As a result, the lenticule could not be removed and the fellow surgeon decided to send the patient home.
To support the surgeon, Dr. Fantozzi traveled to the clinic 20 days later and helped to successfully dissect the lenticule in the upper plane. The lesson here, Dr. Fantozzi said, is that if the beginner SMILE surgeon is in trouble, “leave the lenticule alone and call an expert.”
Pearls to Minimize Suction Loss
Dan Z. Reinstein, MD, MA(Cantab), FRCSC, DABO, FRCOphth, FEBO, of the London Vision Clinic, provided pearls for minimizing suction loss during SMILE—a very rare event. These included constantly talking to the patient during surgery, providing patients with clear instructions regarding the fixation light (ie, “Look at the green light.” “Do not follow the green light.”), and intense monitoring of any eye movement or torque during cutting. Dr. Reinstein also suggested having a high sensitivity for aborting the cut when necessary. In the very rare event that suction loss does occur, following a protocol will ensure the procedure can still be completed.
Six SMILE Enhancement Techniques Reviewed
Another hot topic at the symposium was how to deal with enhancements after SMILE. Glenn I. Carp, MBBCh, FCOphth(SA), of the London Vision Clinic, reviewed six retreatment options: PRK, sidecut only, Circle, thin-flap LASIK, sub-cap lenticule extraction, and intrastromal keratotomy. The last three, Dr. Carp said, are currently off-label treatments. PRK can be used as long as the patient’s final pachymetry is more than 350 µm, but the associated disadvantages are pain, the risk of haze, slow visual recovery, and an initial hyperopic over-correction. The advantage of a sidecut-only approach to retreatment, converting the cap into a flap, is that it is easy to lift; however, it forces the flap to be as thick as the cap. The Circle technique converts the cap into a flap with a larger diameter. This is a good option for thin-cap SMILE cases, Dr. Carp said.
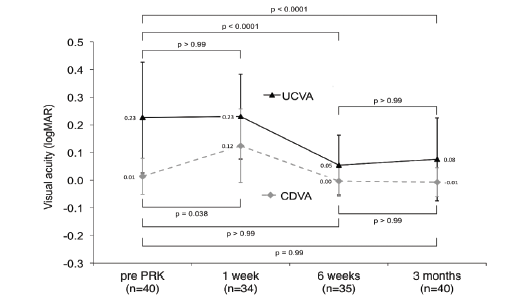
Figure 1. UCVA at 3 months postoperative.
Surface Ablation to Treat Residual Refractive Errors
Also discussing enhancements, Martin Dirisamer, MD, PhD, of Ludwig-Maximilians-University of Munic, Germany, said that PRK with mitomycin-C application is a safe and effective way to treat residual refractive errors after SMILE. In his clinic, the enhancement rate after SMILE is very low, at 2.2%. He recently studied the outcomes of this enhancement technique in 28 touchup procedures, with a mean time to retreatment of 9.82 ±5.27 months, and found a significant improvement in UCVA at 3 months postoperative (Figure 1). Professor Dirisamer cautioned against using the ASA (aspheric optimized) profile, due to the tendency to overcorrect the refractive error.
Clinical Decision Pathway
Fernand de Wilde, MD, of the Eyecenter Latem, Belgium, also underwent PRESBYOND Laser Blended Vision because he felt that the surgery had the least amount of risks and the best chance for optimal visual performance. By age 55, he had become frustrated by his need of spectacles for reading and driving. After losing a pair of his readers during the 2016 ZEISS European Refractive Laser Symposium, Dr. de Wilde vowed to undergo a procedure to help alleviate his presbyopic symptoms.
His PRESBYOND procedure, performed by Dr. Reinstein in November 2016, lasted 11 minutes and was completely pain-free. He said that having Dr. Reinstein talk to him throughout the procedure was comforting. On day 1 postoperative, Dr. de Wilde’s UCVA was 20/40+1 in his right eye, 20/20 in his left, and 20/16 binocularly. On topography, the treatment was well-centered, and the corneal spherical aberrations were close to 0 in both eyes (Figure 2).
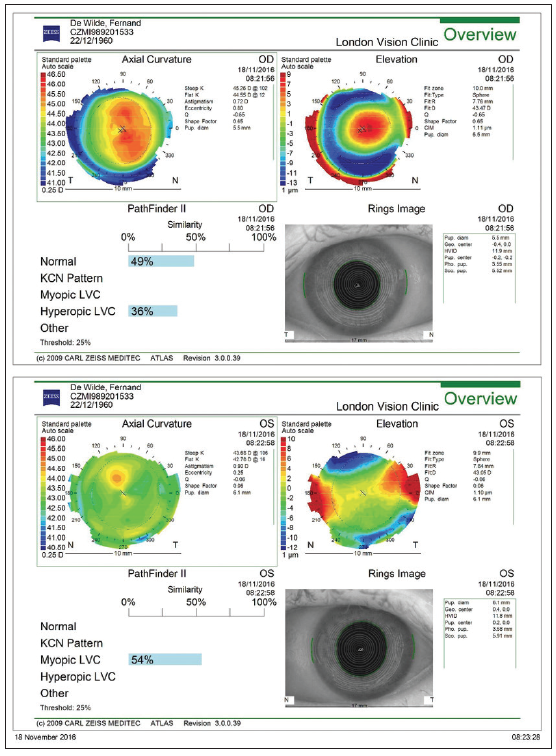
Figure 2. Topography of Dr. de Wilde’s eyes at 1 day postoperative.
Dr. de Wilde also experienced some dry eye symptoms; however, by 6 weeks postoperative, his dry eye symptoms had improved. He mainly attributed the dry eye to the fact that he had mild Meibomian gland dysfunction preoperatively. Now that he has had PRESBYOND, he feels that he can more enthusiastically suggest the procedure to his patients and acknowledges that his surgical approach to presbyopia treatment has changed over the past few years.
Why and When Trifocal IOLs Provide Best Outcomes
In addition to discussions on PRESBYOND Laser Vision Correction, another hot topic during the managing presbyopia session of the 2017 ZEISS European Refractive Laser Symposium was lens-based strategies to presbyopic intervention. “The best solution today to [compensate for] presbyopia despite the most advanced refractive surgery is trifocal IOL technology,” Matteo Piovella, MD, of the Centro Microchirurgia Ambulatoriale, Monza, Italy, said during the symposium.

Figure 3. Seven of the eight surgeons who spoke at the Mastering Presbyopia Session had their eyes treated.
The reason, he said, is that the quality of vision that patients can obtain with a trifocal IOL is exceptionally high. It is for this reason that Dr. Piovella himself has undergone bilateral trifocal IOL implantation with the AT LISA tri (ZEISS) in his right eye and the AT LISA tri toric in his left.
Dr. Piovella had high myopia (-8.00 D) and admits he was not a good candidate; however, he researched the data and results and decided that the AT LISA tri platform would work for him. In July 2014, H. Burkhard Dick, MD, PhD, performed the cataract surgery procedure. Dr. Piovella said that he has been perfectly happy with the results and is glad that he chose the AT LISA tri and AT LISA tri toric for his own eyes.
Dr. Piovella said that, to achieve the best outcomes with trifocal IOLs, it is crucial to select not only the right candidate but the right eye. Efficient, “personalized” biometry is the key to achieving this goal. In his experience, the best postoperative results are seen in eyes that provide the opportunity to:
- Apply high-standard biometry, in order to get high-precision results for IOL calculation;
- Achieve 20/20 visual acuity after surgery; and
- Reach emmetropia after surgery.
Dr. Piovella said that he has never explanted a trifocal IOL, and he believes that it is because he has taken the time to select the right kind of eye for the implant. He also cautioned that one must be careful using the lens, like any premium IOL technology, in eyes with high myopia and high hyperopia.
In Dr. Piovella’s experience, trifocal IOLs are less sensitive to small amounts of postoperative refractive errors; provide the best near, intermediate, and distance vision of any lens technology; and, in his practice, have replaced first-generation multifocal IOL technologies.
Putting It All Together
As demonstrated during the 2017 ZEISS European Refractive Laser Symposium, today’s patients have many options to consider in their quest for presbyopia compensation. Because all of these procedures provide the opportunity for excellent postoperative outcomes, setting one apart from the rest could be challenging.
One thing that has the potential to leave a lasting impact on patients is when surgeons are confident enough to undergo surgery themselves—much like the surgeons who spoke at the symposium in Paris.



