


A 14-year-old girl was referred by her optometrist, who had noticed unusual pigmentation in the periocular skin and conjunctiva of the patient’s left eye. A slit-lamp biomicroscopic examination found ipsilateral grayish-blue hyperpigmentation of the periocular skin, patchy pigmentation of the conjunctiva and sclera, and heterochromia. The patient stated that this asymptomatic finding had been present since birth. Gonioscopy revealed open angles in all quadrants with no excessive pigmentation.
A fundus examination showed a violaceous hue due to hyperpigmentation of the choroidal vasculature in the left eye and a normal appearance in the right eye. The patient’s medical and family history was unremarkable, and no pigmentation was visible in the oral cavity. A systemic examination was noncontributory.
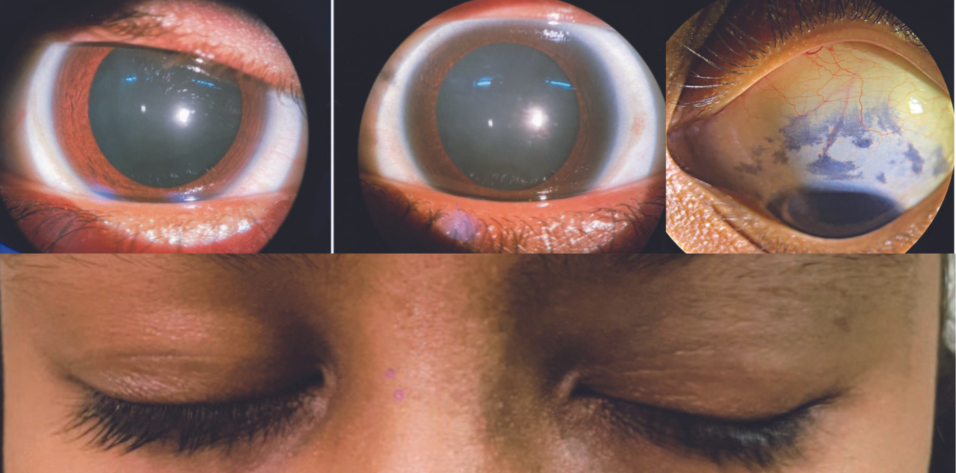
Based on the clinical and imaging findings (Figures 1–4), our diagnosis was nevus fusco-caeruleus ophthalmo-maxillaris/oculodermal melanocytosis, or Nevus of Ota, in the left eye. We explained the nature of the disorder, its natural course, and the importance of regular follow-up visits to the patient and her parents.
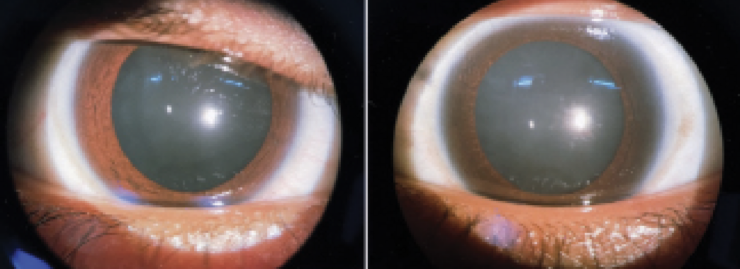
Figure 1. The patient’s left eye exhibits heterochromia.
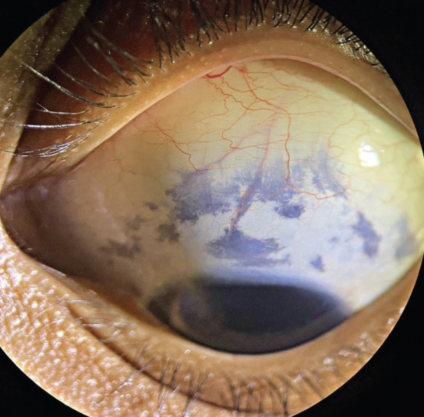
Figure 2. Conjunctival and episcleral pigmentation in the left eye.

Figure 3. Grayish-blue hyperpigmentation of the periocular skin of the left eye.

Figure 4. Ipsilateral hyperpigmented skin around the left eye (A). Left eye heterochromia along with superior episcleral and conjunctival pigmentation (B). Left eye episcleral pigmentation on the inferior side (C). Left eye choroidal vasculature exhibiting violaceous hue due to hyperpigmentation (D).
ABOUT NEVUS OF OTA
Nevus of Ota is a benign melanosis characterized by blue-gray or brown, irregular, often spotted skin discoloration that bears a resemblance to a powder-blast burn and is located on the face. The discoloration occurs in the distribution of the ophthalmic and maxillary branches of the trigeminal nerve (ie, the forehead, periorbital area, temple, and cheek regions), including the sclera, the fundus, and occasionally the mandibular divisions of the facial nerve.1
The term fusco-caeruleus connotes a dark dusky-slate-tan-brown-purple-sky blue color. The bluish color results from the scattering of light by dermal melanin (Tyndall phenomenon). Macules are confluent, nonhairy, and flat with poorly defined margins. The color may also vary slightly depending on factors such as weather conditions, hormones, and illness. It is believed to occur owing to migration arrest of melanocytes on their way to the epidermis from the neural crest.
EPIDEMIOLOGY
The prevalence of Nevus of Ota is greatest among individuals of Asian and African descent; it affects approximately 0.014% to 0.034% of these populations.2 The condition is usually unilateral but occurs bilaterally in 5% of cases.
About 50% of lesions are present at birth, and the remainder appear during puberty. Nevus of Ota has a female preponderance. The disorder is lifelong and generally benign. The risk of malignant melanoma is much higher among White individuals compared to other racial and ethnic groups.
EVALUATION AND TREATMENT
Diagnosis
A diagnosis of Nevus of Ota is based mainly on the clinical examination and history. There is no definitive diagnostic test to confirm the disorder. A thorough ophthalmic examination, including gonioscopy and a fundus examination, should be performed.
Patients’ vision is not particularly impaired by the pigmentary disorder, but they are at increased risk of malignant melanoma and glaucoma.3
A skin biopsy is required if the overlying skin develops ulceration or there is a variation in pigmentation with the development of papules.
Differential Diagnosis
The differential diagnosis of Nevus of Ota includes nevus flammeus, café au lait spots, contusion or suffusion, ochronosis, circumscribed precancerous melanosis, chloasma, argyria, superficial malignant melanoma, congenital conjunctival pigmentation, diffuse flat nevus of the conjunctiva, and precancerous melanosis of the eye.
Prognosis
The prognosis of these patients is good. A majority of them present to an eye care provider owing to pigmentation of the sclera and iris. The most effective approach for cosmetic treatment of skin lesions associated with Nevus of Ota is laser therapy.4 Treatment is thought to destroy the melanocytes that mediate the bluish hyperpigmented sections on the skin.
Follow-up
Patients should follow up with an ophthalmologist annually to rule out ocular complications.
1. Kopf AW, Weidman AI. Nevus of Ota. Arch Dermatol. 1962;85:195-208.
2. Sekar S, Kuruvila M, Pai HS. Nevus of Ota: a series of 15 cases. Indian J Dermatol Venereol Leprol. 2008;74:125-127.
3. Cronemberger S, Calixto N. Freitas HL. Nevus of Ota: clinical – ophthalmological findings. Revista Brasileira de Oftalmologia. 2011;70: 278-283.
4. Bhattacharya SK, Girgla HS, Singh G. Nevus of Ota. Int J Dermatol. 1973;12(6):344-347.