




The evolution of cataract surgical techniques has increased the procedure’s efficiency and improved outcomes, but intra- and postoperative complications can affect the vitreous and retina. Most of these conditions may be successfully comanaged by the cataract surgeon in conjunction with a retina surgeon. The best outcomes are achieved when the cataract surgeon can assess the patient’s pre- and intraoperative risk factors for retinal complications and when prompt diagnosis and management with a retina specialist are initiated.
PSEUDOPHAKIC CYSTOID MACULAR EDEMA
Cystoid macular edema (CME) is the most common cause of vision loss after cataract surgery.1 Historically referred to as Irvine-Gass syndrome, pseudophakic CME was described by Irvine in 1953, and the fluorescein findings were later detailed by Gass.2,3 The reported incidence of CME varies from 0.1% to 11% of eyes after uneventful cataract surgery.1,4-9 Postoperatively, inflammatory mediators are upregulated in both the aqueous and the vitreous, leading to a breakdown of the blood-retinal barrier and an increase in vascular permeability.10
Risk factors for CME include vitreous loss; retained lens fragments; anterior vitrectomy; iris trauma; posterior capsular rupture; IOL dislocation; implantation of an anterior chamber or iris-fixated IOL; presence of epiretinal membrane; and a history of diabetic macular edema,11 uveitis, retinal vein occlusion, or retinal detachment repair.12 In order to reduce the risk of postoperative CME, all preexisting retinal conditions should be controlled before cataract surgery. Eyes with diabetic retinopathy or diabetic macular edema should be evaluated and treated as appropriate; often, an anti-VEGF injection will be required 1 to 2 weeks before surgery.13 Adequate control of intraocular inflammation for at least 3 months before the cataract procedure is recommended for patients with uveitis.6
When to comanage. CME typically occurs between 4 and 12 weeks after surgery, with a peak incidence at 4 to 6 weeks postoperatively.5-7,10 Topical NSAIDs may be administered postoperatively as prophylaxis in patients undergoing cataract surgery who are at high risk of developing CME.9,14-16 When diagnosed after cataract surgery in a patient whose procedure was otherwise uncomplicated, treatment for CME typically consists of topical corticosteroid and NSAID eye drops, and this treatment may be initiated by the cataract surgeon. Data suggest that these medications work synergistically and that outcomes are superior with combination therapy compared with monotherapy.17 If the cataract procedure was complicated or there was a preexisting risk factor, the cataract surgeon may wish to consider initiating treatment for CME and making a prompt referral to a retina specialist.
When to refer. If CME persists despite topical treatment, a referral to a retinal specialist is warranted. At this point, periocular or intravitreal corticosteroids and anti-VEGF treatment are recommended. An early referral and comanagement with a retina specialist should be considered if the etiology of CME is related to complicated cataract surgery and there is evidence of abnormal vitreous adhesions, vitreous incarceration at the incision, retained lens material, vitreomacular traction, or an epiretinal membrane.
RETAINED LENS FRAGMENTS
Retained lens fragments (Figure 1) complicate 0.18% to 1.1% of cataract surgeries.18-22 Both the timing of medical and surgical treatment and the collaborative involvement of an anterior segment surgeon and a vitreoretinal surgeon are critical in managing this condition. Complications related to retained lens fragments include elevated IOP, intraocular inflammation, corneal edema, CME, and retinal detachment.
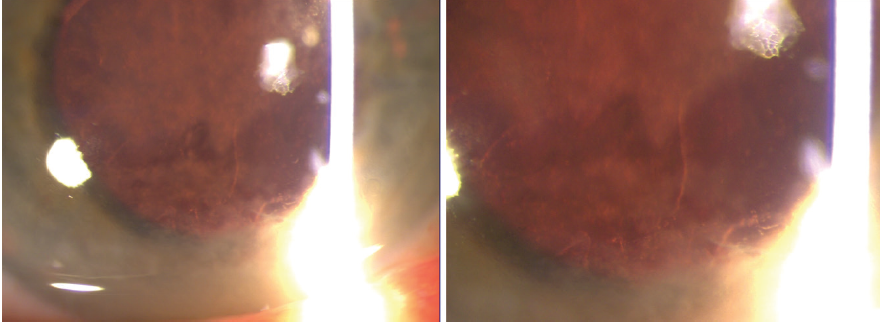
Figure 1. Slit-lamp photographs demonstrating cortical lens fragments in the anterior chamber.
A major factor in avoiding retained lens fragments is preoperatively identifying potential risk factors such as a history of trauma, zonular dehiscence, pseudoexfoliation, high myopia, prior eye surgery, a history of retinopathy of prematurity, a brunescent cataract, tamsulosin use, prior vitrectomy, and multiple prior intravitreal injections.23-26 Intraoperatively, posterior capsular rupture should be identified promptly, and if vitreous prolapse occurs, an anterior vitrectomy should be performed (Editor’s note: For more information on anterior vitrectomy, see “Strategies for Anterior Vitrectomy,” and “Anterior Vitrectomy: Concepts From a Retina Specialist.”) Anterior segment surgeons should not attempt to remove material from the vitreous cavity.
Suturing all incisions and minimizing corneal edema for potential future surgery are important steps. IOL insertion is advisable if there is adequate capsular support without vitreous prolapse in the anterior chamber. Each case must be assessed individually; the severity of inflammation, the amount and type (nuclear vs cortical) of retained lens material, and IOP may influence the management strategy.
When to comanage. The cataract surgeon may initiate medical management with topical drops to control inflammation and IOP. Small cortical lens fragments may dissolve with topical corticosteroids, supplemented on occasion with dilating and IOP-reducing eye drops.
When to refer. Pars plana vitrectomy is indicated to remove nuclear and large cortical pieces. Persistent IOP elevation also necessitates more urgent surgical intervention. In these situations, most retina specialists recommend a vitrectomy within 2 to 3 weeks to improve outcomes and reduce the risks associated with elevated IOP. It may be necessary to delay surgical intervention, however, if there is insufficient media clarity such as the presence of significant corneal edema that must be treated to permit a safe vitrectomy. Patients who have retained lens fragments after cataract surgery should be monitored for the development of delayed vision loss from complications such as CME or retinal detachment.
DISLOCATED IOL
Most IOLs are placed securely in the capsular bag. On occasion, however, an IOL can become dislocated and require secondary intervention (Figure 2). The incidence of IOL dislocation after cataract surgery ranges from 0.3% to 1%.27,28 Late spontaneous IOL dislocation occurs because of zonular weakness or dehiscence. Risk factors include trauma, prior vitreoretinal surgery, pseudoexfoliation syndrome, connective tissue disorders, uveitis, axial myopia, and retinitis pigmentosa.29
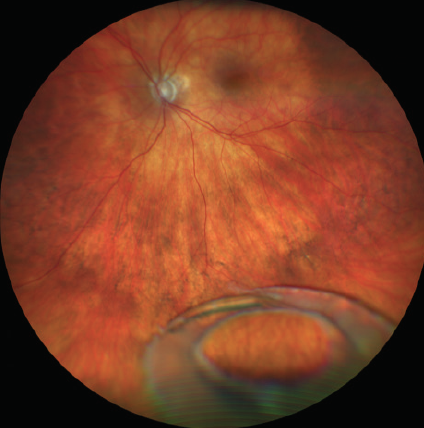
Figure 2. A fundus photograph showing a dislocated IOL resting on the retinal surface.
When to comanage. The anterior segment surgeon may choose to manage a partially subluxated or decentered IOL alone if it has not prolapsed into the vitreous cavity, vitreous prolapse has not occurred, and there is no concurrent retinal pathology. There are many techniques for refixating or recentering an IOL via a limbal surgical approach. Depending on the remaining capsular support and ocular factors, the surgeon may choose to open the capsular bag or sulcus with an OVD and then either reposition and refixate the IOL to the iris or sclera or remove and replace the IOL.
When to refer. A referral to a retina specialist is necessary when an IOL has completely dislocated posteriorly into the vitreous or onto the retinal surface. A pars plana vitrectomy is safer for removing or repositioning the IOL. These cases can be managed either by a retina surgeon alone, as simultaneous procedures, or by both a retina surgeon and the anterior segment surgeon, as sequential procedures.
For the collaborative approach, the retina specialist performs the vitrectomy and brings the lens into the anterior chamber (see Watch It Now). The anterior segment surgeon can then either remove the lens or perform iris or scleral fixation. If the lens is removed, the cataract surgeon can implant a replacement IOL in the anterior chamber or use scleral fixation.
A dislocated IOL is brought into the anterior chamber from the posterior cavity via a pars plana vitrectomy and then removed through a scleral tunnel.
RETINAL DETACHMENT
Retinal detachment is an infrequent but sight-threatening complication of cataract surgery. Vitreous changes occurring after cataract surgery may lead to posterior vitreous detachment, which increases the risk of a retinal tear or detachment. The presence of floaters and photopsia and reported visual field or acuity changes can indicate retinal detachment. A dilated examination of the retina is mandatory and includes an evaluation for tobacco dust or pigmented cells in the anterior vitreous (ie, Schaffer’s sign), a Weiss ring signifying vitreous separation from the optic nerve, and the peripheral retina for tears or detachment.
When to refer. If a retinal tear or detachment is noted or symptoms are unremitting, an immediate referral to a retina specialist is indicated.
ENDOPHTHALMITIS
Postoperative endophthalmitis can cause severe and potentially irreversible vision loss. This complication occurs after 0.04% to 0.2% of cataract surgeries.22,30-33 An examination may reveal conjunctival injection, corneal edema, intraocular inflammation with anterior and vitreous cells or debris, hypopyon, or fibrin. In severe cases, the red reflex may be blunted, and the view of the posterior segment may be limited. Risk factors for endophthalmitis include prolonged surgery, posterior capsular rupture, vitreous loss, placement of a secondary IOL, wound leak or hypotony, vitreous incarceration, and combined surgery (eg, glaucoma and cataract procedures).22,34
In addition to early diagnosis, the cataract surgeon plays an important role in the prevention of postoperative endophthalmitis. Several steps can be taken to reduce the risk. The most effective method of preoperative antisepsis is the application of 5% povidone-iodine solution to the corneal surface, conjunctival sac, and periocular surface.35-37 A 3-minute exposure time before the initiation of surgery is effective.38 Topical and intracameral antibiotics are also widely used for prophylaxis. In a prospective randomized study by the ESCRS, the risk of postoperative endophthalmitis was nearly five times higher in patients who did not receive intracameral antibiotics compared with those who received intravitreal cefuroxime at the end of cataract surgery.39 Intravitreal vancomycin prophylaxis in sequential cataract surgery is not recommended, however, because of the risk of hemorrhagic occlusive retinal vasculitis.40
When to refer. A patient with suspected endophthalmitis should be immediately referred to a retina specialist for evaluation and treatment.
CONCLUSION
Most complications occurring after cataract surgery may be effectively comanaged by the anterior segment surgeon and a retina surgeon. Teamwork is the cornerstone of caring for a patient who experiences vitreoretinal complications after cataract surgery. Expediting referral in complicated cases after the appropriate initial diagnostic and therapeutic steps have been taken is essential for achieving the best visual outcomes.
1. Flach AJ. The incidence, pathogenesis and treatment of cystoid macular edema following cataract surgery. Trans Am Ophthalmol Soc. 1998;96:557-634.
2. Irvine SR. A newly defined vitreous syndrome following cataract surgery. Am J Ophthalmol. 1953;36(5):499-619.
3. Gass JD, Norton EW. Fluorescein studies of patients with macular edema and papilledema following cataract extraction. Trans Am Ophthalmol Soc. 1966;64:232-249.
4. Henderson BA, Kim JY, Ament CS, Ferrufino-Ponce ZK, Grabowska A, Cremers SL. Clinical pseudophakic cystoid macular edema. Risk factors for development and duration after treatment. J Cataract Refract Surg. 2007;33(9):1550-1558.
5. Loewenstein A, Zur D. Postsurgical cystoid macular edema. Dev Ophthalmol. 2010;47:148-159.
6. Bélair ML, Kim SJ, Thorne JE, et al. Incidence of cystoid macular edema after cataract surgery in patients with and without uveitis using optical coherence tomography. Am J Ophthalmol. 2009;148(1):128-135.e2.
7. Perente I, Utine CA, Ozturker C, et al. Evaluation of macular changes after uncomplicated phacoemulsification surgery by optical coherence tomography. Curr Eye Res. 2007;32(3):241-247.
8. Shelsta HN, Jampol LM. Pharmacologic therapy of pseudophakic cystoid macular edema: 2010 update. Retina. 2011;31(1):4-12.
9. Wolf EJ, Braunstein A, Shih C, Braunstein RE. Incidence of visually significant pseudophakic macular edema after uneventful phacoemulsification in patients treated with nepafenac. J Cataract Refract Surg. 2007;33(9):1546-1549.
10. Benitah NR, Arroyo JG. Pseudophakic cystoid macular edema. Int Ophthalmol Clin. 2010;50(1):139-153.
11. Baker CW, Almukhtar T, Bressler NM, et al, Diabetic Retinopathy Clinical Research Network Authors/Writing Committee. Macular edema after cataract surgery in eyes without preoperative central-involved diabetic macular edema. JAMA Ophthalmol. 2013;131(7):870-879.
12. Chu CJ, Johnston RL, Buscombe C, Sallam AB, Mohamed Q, Yang YC, United Kingdom Pseudophakic Macular Edema Study Group. Risk factors and incidence of macular edema after cataract surgery a database study of 81984 eyes. Ophthalmology. 2016;123(2):316-323.
13. Kohnen T. Prevention of cystoid macular edema after cataract surgery in diabetic patients. J Cataract Refract Surg. 2018;44(7):795-796.
14. Wittpenn JR, Silverstein S, Heier J, Kenyon KR, Hunkeler JD, Earl M, Acular LS for Cystoid Macular Edema (ACME) Study Group. A randomized, masked comparison of topical ketorolac 0.4% plus steroid vs steroid alone in low-risk cataract surgery patients. Am J Ophthalmol. 2008;146(4):554-560.
15. Yavas GF, Öztürk F, Küsbeci T. Preoperative topical indomethacin to prevent pseudophakic cystoid macular edema. J Cataract Refract Surg. 2007;33(5):804-807.
16. Almeida DRP, Johnson D, Hollands H, et al. Effect of prophylactic nonsteroidal antiinflammatory drugs on cystoid macular edema assessed using optical coherence tomography quantification of total macular volume after cataract surgery. J Cataract Refract Surg. 2008;34(1):64-69.
17. Heier JS, Topping TM, Baumann W, Dirks MS, Chern S. Ketorolac versus prednisolone versus combination therapy in the treatment of acute pseudophakic cystoid macular edema. Ophthalmology. 2000;107(11):2034-2038.
18. Mahr MA, Lum F, Fujino D, Kelly SP, Erie JC. Return to the operating room for removal of retained lens fragments after cataract surgery: IRIS Registry (Intelligent Research in Sight) analysis. Ophthalmology. 2020;127(5):698-699.
19. Aasuri MK, Kompella VB, Majji AB. Risk factors for and management of dropped nucleus during phacoemulsification. J Cataract Refract Surg. 2001;27(9):1428-1432.
20. Jaycock P, Johnston RL, Taylor H, et al. The Cataract National Dataset electronic multi-centre audit of 55,567 operations: updating benchmark standards of care in the United Kingdom and internationally. Eye (Lond). 2009;23(1):38-49.
21. Pande M, Dabbs TR. Incidence of lens matter dislocation during phacoemulsification. J Cataract Refract Surg. 1996;22(6):737-742.
22. Pershing S, Lum F, Hsu S, et al. Endophthalmitis after cataract surgery in the United States: a report from the Intelligent Research in Sight Registry, 2013–2017. Ophthalmology. 2020;127(2):151-158.
23. Lee AY, Day AC, Egan C, et al. Previous intravitreal therapy is associated with increased risk of posterior capsule rupture during cataract surgery. Ophthalmology. 2016;123(6):1252-1256.
24. Chang D. Phacoemulsification in high risk cases. In: Wallace RB, ed. Refractive Cataract Surgery and Multifocal IOLs. Slack; 2001:121-136.
25. Gilliland GD, Hutton WL, Fuller DG. Retained intravitreal lens fragments after cataract surgery. Ophthalmology. 1992;99(8):1263-1267; discussion 1268-1269.
26. Borne MJ, Tasman W, Regillo C, Malecha M, Sarin L. Outcomes of vitrectomy for retained lens fragments. Ophthalmology. 1996;103(6):971-976.
27. Gimbel HV, Condon GP, Kohnen T, Olson RJ, Halkiadakis I. Late in-the-bag intraocular lens dislocation: incidence, prevention, and management. J Cataract Refract Surg. 2005;31(11):2193-2204.
28. Mönestam E. Frequency of intraocular lens dislocation and pseudophacodonesis, 20 years after cataract surgery – a prospective study. Am J Ophthalmol. 2019;198:215-222.
29. Ascaso FJ, Huerva V, Grzybowski A. Epidemiology, etiology, and prevention of late IOL-capsular bag complex dislocation: review of the literature. J Ophthalmol. 2015;2015:805706.
30. Packer M, Chang DF, Dewey SH, et al; ASCRS Cataract Clinical Committee. Prevention, diagnosis, and management of acute postoperative bacterial endophthalmitis. J Cataract Refract Surg. 2011;37(9):1699-1714.
31. Taban M, Behrens A, Newcomb RL, et al. Acute endophthalmitis following cataract surgery: a systematic review of the literature. Arch Ophthalmol. 2005;123(5):613-620.
32. West ES, Behrens A, McDonnell PJ, Tielsch JM, Schein OD. The incidence of endophthalmitis after cataract surgery among the U.S. Medicare population increased between 1994 and 2001. Ophthalmology. 2005;112(8):1388-1394.
33. Lundström M, Wejde G, Stenevi U, Thorburn W, Montan P. Endophthalmitis after cataract surgery: a nationwide prospective study evaluating incidence in relation to incision type and location. Ophthalmology. 2007;114(5):866-870.
34. Galor A, Goldhardt R, Wellik SR, Gregori NZ, Flynn HW. Management strategies to reduce risk of postoperative infections. Curr Ophthalmol Rep. 2013;1(4):161-168.
35. Wu PC, Li M, Chang SJ, et al. Risk of endophthalmitis after cataract surgery using different protocols for povidone-iodine preoperative disinfection. J Ocul Pharmacol Ther. 2006;22(1):54-61.
36. Stranz CV, Fraenkel GE, Butcher AR, Esterman AJ, Goggin MJ. Survival of bacteria on the ocular surface following double application of povidone-iodine before cataract surgery. Eye (Lond). 2011;25(11):1423-1428.
37. Ferguson AW, Scott JA, McGavigan J, et al. Comparison of 5% povidone-iodine solution against 1% povidone-iodine solution in preoperative cataract surgery antisepsis: a prospective randomised double blind study. Br J Ophthalmol. 2003;87(2):163-167.
38. Nguyen CL, Oh LJ, Wong E, Francis IC. Povidone-iodine 3-minute exposure time is viable in preparation for cataract surgery. Eur J Ophthalmol. 2017;27(5):573-576.
39. Endophthalmitis Study Group, European Society of Cataract & Refractive Surgeons. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg. 2007;33(6):978-988.
40. Witkin AJ, Shah AR, Engstrom RE, et al. Postoperative hemorrhagic occlusive retinal vasculitis: expanding the clinical spectrum and possible association with vancomycin. Ophthalmology. 2015;122(7):1438-1451.