
In my opinion, the next frontier in premium cataract surgery is to resolve three outstanding problems: (1) aligning IOLs to the visual axis; (2) controlling for lens tilt and x-y decentration; and (3) ensuring that an IOL lies in an anterior-posterior direction. If we can resolve these issues, then we can refine our outcomes even further and serve those patients who get an unexpected refractive result. The FEMTIS® IOL Family (Teleon Surgical) presents a distinctive design and optical platform that may offer us novel solutions to these problems.
The design of the FEMTIS IOL is unique among available IOL platforms in that it attaches to the anterior capsulorhexis. Using four clip haptics (Figure 1), the lens reliably fixates in the correct position inside the eye, rather than settling in the space vacated by the crystalline lens (Figure 2). This means that if we make a capsulorhexis that is perfectly aligned with the visual axis—something optimally achieved with a femtosecond laser—then the FEMTIS will be aligned with the visual axis. In contrast, IOLs centered in the capsular bag will align themselves with the equator of the capsular bag, which may or may not correlate with the visual axis.

Figure 1. In addition to its two modified plate haptics, the FEMTIS platform contains four clip haptics (two large, two small) that attach to the anterior capsulorhexis (pink tint).

Figure 2. A rendering of the FEMTIS IOL’s attachment to the anterior capsulorhexis.
Furthermore, current multifocal and extended depth-of-focus (EDOF) lens designs are engineered to allow for decentration from the visual axis. If the deviation exceeds approximately 600 µm, patients may start to experience unwanted visual phenomena. The FEMTIS lens largely avoids these phenomena by, again, aligning perfectly with the visual axis every time when it is combined with the precise alignment of a femtosecond-created capsulotomy.
The Advantages of a Segmental Multifocal Optic Design
The FEMTIS® IOL Family, which includes the monofocal FEMTIS, the FEMTIS Comfort, the FEMTIS Comfort Toric, the FEMTIS Mplus, and the the FEMTIS Mplus Toric, is based on an optical design that has been in use for more than a decade, first in the LENTIS® IOL (Teleon Surgical) platform. Rather than using diffractive technology to generate near vision, the segmental optic concept of FEMTIS Comfort and FEMTIS Mplus is purely refractive. Its defocus curve doesn’t show sharp peaks for 2 or 3 points of vision, as is seen with a bifocal or trifocal lens. Intrinsic to the asymmetric segmental refractive technology are a smooth defocus curve and transition-free central optics. Its optical segmentation enables a continuous distribution of light throughout the intermediate viewing area, which is called the varifocal effect. Thus, the FEMTIS optic design uses light more efficiently, losing only about 8% versus the 15% of light lost by diffractive multifocal lenses. With such light efficiency, patients achieve good functional vision and a wide range of vision without having to accept the compromise of unwanted visual phenomena. In contrast, diffractive multifocals have a significant compromise: haloing at night. It happens with all diffractive IOL technologies; the only question is how much it bothers the patient. Importantly, the FEMTIS IOL technology does not produce halos.1 These lenses are good for patients because they are effective; they’re good for surgeons, because they make patients happy; and they are good for our practices, because they eliminate chair time discussing halos.
Handling and Placing the FEMTIS IOL in the Capsulorhexis
Whenever I teach surgeons how to implant FEMTIS IOLs, they’re always surprised at how easy it is. We inject the lens into the capsular bag under viscoelastic, just like a standard lens. After removing the viscoelastic from behind the lens and adding a little more in front of the lens, we attach the four enclavation flanges onto the anterior edge of the capsulorhexis. The entire technique adds maybe 20 to 40 seconds to the total surgical time.
Rotational Stability, Yet Easy Manipulation
The FEMTIS IOL comes in two toric models, the FEMTIS Comfort® toric and the FEMTIS Mplus® toric, which are easy to use. Even after attaching them to the anterior capsulorhexis via the clip haptics, it’s easy to rotate them in either direction to accurately align with the toric axis, far better than a lens in the capsular bag. Once rotated, the FEMTIS toric IOL will stay exactly where we leave it (Figures 3 through 5). The predictability of alignment with the correct toric axis is one of the strongest features of the FEMTIS toric IOL, especially when used with a digital marker system. Yet, if we need to re-enter the eye to realign the IOL, then the lens is very accessible; we can touch it and reposition it quite easily.

Figure 3. In the FEMTIS multicenter study, the lens’ degree of rotation was very low. (Data adapted from Auffarth GU, et al. Stability and visual outcomes of the capsulotomy-fixated Femtis-IOL after automated femtosecond laser-assisted anterior capsulotomy. Am J Ophthalmol. 2021.)
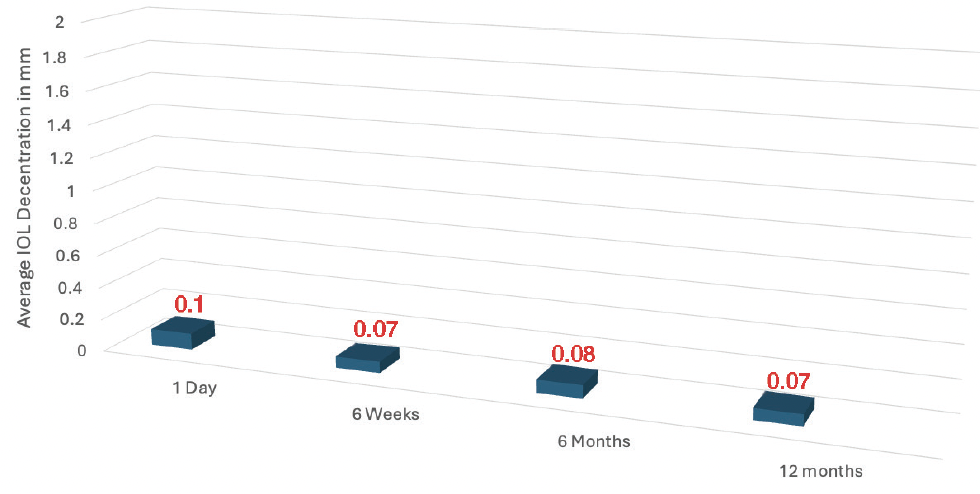
Figure 4. In the FEMTIS multicenter study, the lens’ amount of decentration was very low. (Data adapted from Auffarth GU, et al. Stability and visual outcomes of the capsulotomy-fixated Femtis-IOL after automated femtosecond laser-assisted anterior capsulotomy. Am J Ophthalmol. 2021.).
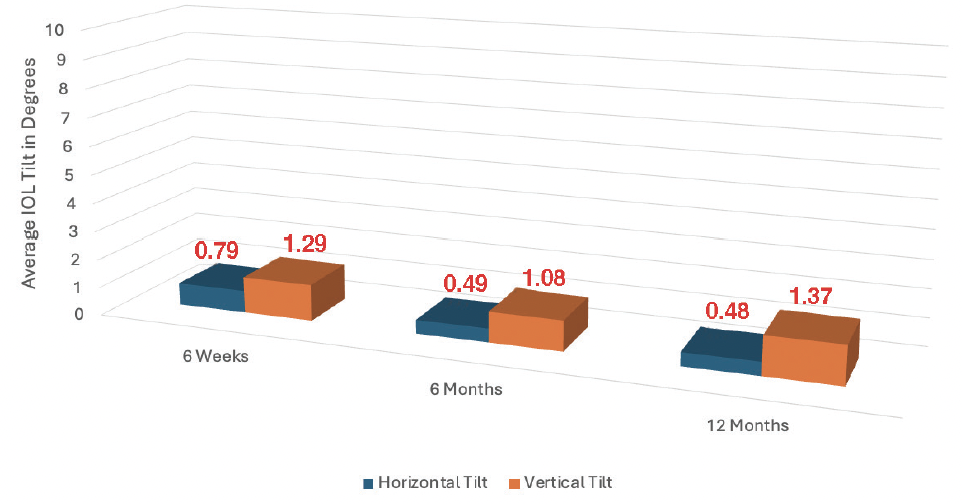
Figure 5. In the FEMTIS multicenter study, the lens’ degree of horizontal and vertical tilt was minimal, even at 12 months postoperatively. (Data adapted from Auffarth GU, et al. Stability and visual outcomes of the capsulotomy-fixated Femtis-IOL after automated femtosecond laser-assisted anterior capsulotomy. Am J Ophthalmol. 2021.)
Patient Satisfaction
We have all encountered post-cataract patients who have great vision on paper, but they are miserable with their quality of vision. The FEMTIS IOL gets excellent feedback, both subjectively and objectively. A colleague and I published our 6-month outcomes of the FEMTIS lens 4 years ago,2 and another group has since published a collaborative, 12-month study with a larger cohort.1 In both those papers, patient satisfaction was very high. And, because of the lens’ superb stability, we can reliably predict its refractive outcome and avoid refractive surprises.
Of course, the visual system of the FEMTIS lens family is different from other IOLs and may require some slight neuroadaptation. To improve its range of vision, I routinely implant the FEMTIS IOL bilaterally, with a near add of 1.50 D in the dominant eye and 3.00 D in the nondominant eye. This strategy provides an extended range of focus by filling out the near and intermediate ranges, yet the distance vision is exactly the same in both eyes. This is not monovision, because both eyes will see 20/20 for distance. Recently, I applied this strategy in a patient who flies a rescue helicopter here in Sydney, which is a highly demanding job that requires him to fly at night in an urban area. With the 1.50 D FEMTIS Comfort in the dominant eye and the 3.00 D FEMTIS Mplus in the other, he is now free of spectacles and has great quality of vision, with no problems flying at night. That’s the kind of outcome I’m looking for and expect to get with this lens.
Considerations for the Long Term
As the evolving pattern is to perform refractive cataract surgery on younger patients, we need to consider the capability of upgrading IOLs. I have already begun encountering this issue. When I started using the FEMTIS Comfort lens, it only came as a 1.50 near add, which gave patients good vision—60% of recipients never wore reading glasses. I’ve since had a couple of patients return 4 or 5 years later desiring spectacle-free reading vision for fine print. After some discussion, I agreed to exchange these patients’ lenses for the 3.00 D FEMTIS Mplus. Even 4 years later, it was very easy to explant the original FEMTIS and implant a new one attached to the capsulorhexis. Moreover, we don’t see the capsular phimosis with the FEMTIS IOLs that is so common after routine cataract surgery. I anticipate that the long-term benefits of the FEMTIS platform will become increasingly valuable to those of us treating an aging population.
1. Auffarth UG, Friedmann E, Breyer D, et al. Stability and visual outcomes of the capsulotomy-fixated FEMTIS-IOL after automated femtosecond laser-assisted anterior capsulotomy. Am J Ophthalmology. 2021;225:27-37.
2. Darian-Smith E, Versace P. Visual performance and positional stability of a capsulorhexis-fixated extended depth-of-focus intraocular lens. J Cataract Refract Surg. 2020;46(2):179-187.

