
When planning cataract surgery in astigmatic eyes, there are several steps necessary to achieve a good outcome. First, preoperative measurements must be precise, and for this I mainly use the Pentacam (Oculus). Second, we must ensure accurate toric IOL alignment. In the OR, my favorite tool is the LENSAR femtosecond laser to mark the axis without manual markings. In my hands, femtosecond laser-assisted cataract surgery (FLACS) achieves the highest reliability by stabilizing the eye and ensuring good registration.
A third key step in astigmatic correction is that the toric IOL needs to stay where it is placed. Especially in myopic eyes, in which the capsular bag is often large, there’s a chance that a bag-fixated IOL will rotate. Therefore, I prefer to implant capsulorhexis-fixated lenses. Having used the FEMTIS® family of IOLs (Teleon Surgical) for the past few years, I have found several advantages to this design. These lenses stay exactly where I place them. Even when I implant a toric FEMTIS model (either the FEMTIS Comfort Toric or the FEMTIS Mplus Toric), I can rotate the lens in either direction inside the eye, using the alignment marks on the optic for guidance (Figure 1). It won’t tilt or become decentered postoperatively. Importantly, the technique to fixate the haptics is fast and easy; it becomes routine after a few cases.
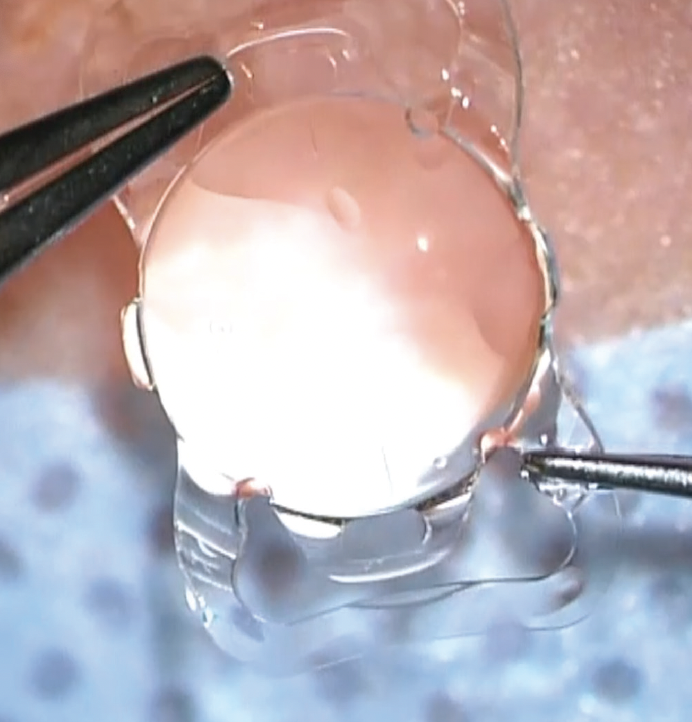
Figure 1. The FEMTIS Comfort Toric IOL with alignment marks.
When cataract surgery candidates want independence from glasses, but they also have astigmatism, we must fix the astigmatism, no matter what IOL technology we choose. We surgeons now have a perfectly matched combination for astigmatic patients who seek premium refractive cataract surgery: fully automated IOL markings, registration, and capsulotomy creation with a femtosecond laser, coupled with the FEMTIS Toric IOLs, which fixate securely to the edge of the capsulorhexis and provide excellent astigmatic correction and segmental multifocal optics on a stable platform.
Case 1: Early Dense Cataracts With Astigmatism
A 42-year-old male patient with metabolic disease presented with early cataracts as well as astigmatism bilaterally. He was a self-described “tech nerd” who worked at a computer each day. He said that he lived in the city and biked to work, and he wanted to be free of glasses for most activities, but he had concerns about the potential visual phenomena with multifocal IOLs, like starbursts, glare, and halos. The rest of his health history was unremarkable. Because he told me that he was willing to wear reading glasses in some limited situations, I suggested the FEMTIS Comfort Toric IOL of 20.00 D, because it would provide good distance visual acuity and moderate any postoperative visual symptoms.
The patient’s preoperative examination revealed a BCVA of 0.2 logMAR in both eyes. His cataracts were mostly in the posterior capsule, and they had developed quite quickly and were fairly dense due to his metabolic disease.
I treated the left eye first, because it was his nondominant eye and its cataract was more severe. Despite the density of the cataract, the zonules were healthy and the surgery and IOL implantation were uncomplicated. Implanting a FEMTIS Comfort Toric IOL is just as easy as a traditional, bag-fixated lens. I use OVD in the same manner, and I stabilize the eye using an instrument made by Geuder AG in Germany, called the “small hammer.” The IOL achieved good positioning (Figure 2), and the patient’s astigmatism OS reduced to 0.25 D. I targeted mini-monovision of approximately -0.7 logMAR, but his final postoperative refraction was closer to -0.8. He was very happy that he was able to read with this eye without glasses.
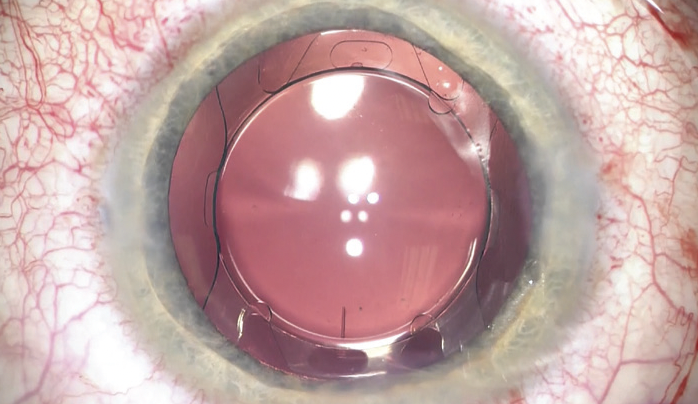
Figure 2. Secure positioning of the FEMTIS Comfort Toric IOL in the nondominant eye of a 42-year-old male patient.
Because this patient was quite nervous during the surgery and had trouble lying still after he received the topical anesthesia, I was grateful to have the eye stabilization and automated marking features of the femtosecond laser. I had no problems with its detection and marking functions, and the capsulotomy was perfectly complete and symmetrical for 360º. I used the dimple-down technique described by Lisa Arbisser, MD, to ensure a free capsulotomy.1 The lens fragmentation went smoothly, after which it was very easy to remove the cataractous lens.
I treated the patient’s right eye 6 weeks later, targeting emmetropia, which he achieved. Again, the surgery was uncomplicated. At his 3-month follow-up visit, the patient told me he was very happy, and that he was only using his reading glasses occasionally for very fine print. For most tasks, he was able to do without them. I attribute this happy outcome to the excellent optics of the FEMTIS Comfort Toric IOL, combined with the capabilities of the FLACS procedure.
Case 2: Significant Astigmatism in a High Myope
A 62-year-old female with a very active lifestyle presented for cataract evaluation. Both eyes were highly myopic, and each had 3.00 D of astigmatism. This patient had worn contact lenses for many years, and now she wanted to be as independent as possible from contacts or spectacles. Because of these three challenges—high astigmatism, high myopia (potentially with a large capsular bag), and the desire for complete spectacle independence—I again selected the FEMTIS Comfort Toric IOL for this patient.
I treated the left (nondominant) eye first, which had an axial length of 26.22 mm. I took preoperative images with the Pentacam (Oculus), which I transferred to the femtosecond laser system at the time of surgery. I targeted a correction of -1.00 D for the left eye and emmetropia in the right eye (axial length, 26.45 mm).
Again, in this case, the laser produced a symmetrical capsulotomy, and then it fragmented the dense nucleus. Due to the amount of astigmatism present, I aimed for mini-monovision to extend the visual benefits of the FEMTIS Comfort Toric IOL. After I treated the second eye, this patient was fully free of glasses.
CONCLUSION
Recent data have shown that the incidence of myopia is increasing throughout the world.2 Myopia poses unique challenges in eyes that need cataract surgery, not the least of which is the size of the capsular bag. I believe that the FEMTIS family of IOLs, with their optic design seated in a capsulorhexis-fixated platform, are uniquely suited to provide these patients the correction and refractive stability they need to achieve the independence from glasses they seek. Using the FLACS technique, we can find the visual axis, place the FEMTIS lenses in a stable location, and make our patients happy with premium multifocal optics, with toric correction if needed.
1. Brothers Arbisser, L. One thing I recently changed. Cataract & Refractive Surgery Today. 2014. https://crstoday.com/articles/2014-jan/one-thing-i-recently-changed. Accessed June 19, 2024
2. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042.

