
In glaucoma management, one of our goals is to individualize the approach to treatment while considering the impact on patients’ quality of life. Yet, in everyday practice, ophthalmologists have historically lacked options with which to achieve that goal. Each of us learned in training, for instance, that patients with primary open-angle glaucoma (POAG) should be started on drops, with more drops added as necessary, before moving to laser if necessary, and finally to incisional surgeries if all else failed. It is important to understand the rationale for this way of treating POAG: prior to the introduction of minimally invasive glaucoma surgery (MIGS), drop therapy was considered sufficient for controlling intraocular pressure (IOP), even if its use was associated with side effects and compliance issues. Furthermore, the only surgical options at our disposal at that time, namely trabeculectomy and glaucoma drainage devices, carried with them appreciable risks of complications and failure.1,2 In short, procedural interventions were considered second- and third-line choices because their use precluded future options.
The introduction of the MIGS class altered the approach to management of POAG (see The Definition of MIGS).3 The favorable safety profile of MIGS relative to traditional incisional surgeries may be a reason that ophthalmic surgeons have increasingly employed MIGS at earlier stages of the disease.4 Indeed, the broad array of MIGS devices and surgeries now available for clinical use has fostered a proactive versus reactive approach to treatment that has come to be known as interventional glaucoma.5 The stated goals of this approach are to reduce and steadily maintain IOP targets, delay or avoid higher-risk surgery, and decrease reliance on patient adherence and compliance, while secondarily resetting the burden on patients by decreasing medication load.5
It is our belief that the array of procedures, devices, and surgeries in the glaucoma treatment armamentarium collectively improve the ability to individualize treatment for each patient while considering the impact on their quality of life. Furthermore, because of the many benefits associated with MIGS, including the prospect of reducing or eliminating medication burden, we should not be constrained by traditional definitions of a successful outcome. Instead, because of the greater ability to personalize care, we can have meaningful conversations with patients regarding their options and consider the risk-benefit profile on an individual basis.
Addressing Multiple Parts of the Aqueous Drainage Pathway
One of the difficulties of treating glaucoma in real-world practice is that we do not know where in the aqueous drainage system the blockage is occurring. We can be partially guided in this regard by the published literature. We know, for instance, that while the trabecular meshwork (TM) is a source of resistance in POAG, the juxtacanalicular region and the Schlemm canal (SC) are also important areas of blockages.6 Furthermore, the collector channels direct flow to the distal drainage system, and ultimately to the episcleral venous system,7 but blockages/herniations or collapse of the SC may block the ostia of the collector channels in eyes with POAG.8 Collectively, this information suggests that one or more of the anatomic structures of the complex aqueous drainage pathway may cause interruptions in flow dynamics. And so, MIGS options that address multiple potential sources of resistance may offer an advantage.
It is notable, then, that the Hydrus® Microstent (Alcon) is associated with a trimodal mechanism of action: it (1) directs aqueous to bypass the TM through the inlet of the device to allow fluid to pass from the anterior chamber into the SC9; (2) it scaffolds the SC to provide permanent patency in the canal to prevent SC collapse9-11; and (3) it maintains patency across a 90° span of the canal,9-11 providing access to multiple collector channels over time with no need to specifically target them for intervention (Figure 1). Made of nitinol, a commonly used material proven to be biocompatible, the Hydrus® Microstent is designed with a slight contour that matches the natural curvature of the SC with three open windows along its 8-mm length that face the anterior chamber, thereby facilitating access to the collector channels.12 Thus, successful implantation of a Hydrus® Microstent mechanically opens and maintains the patency of 90° of SC, which restores aqueous flow. By contrast, bypassing the canal with a focal stent may be insufficient to counteract a collapse of the SC.13

Figure 1. Mechanisms of action for Hydrus® Microstent.
This trimodal mechanism of action and other considerations appear to have contributed to superior outcomes when Hydrus® + cataract surgery (CS) was compared to CS alone in the HORIZON pivotal trial.11,14,15 The important data from this study are reviewed elsewhere in this monograph (see Highlighting Key Data from HORIZON After 2 and 5 Years of Follow-up on page 6). Briefly, Hydrus® Microstent received regulatory approval on the basis of findings from the first 2 years of the study, which demonstrated a high percentage of patients with at least 20% reduction in mean washed-out diurnal IOP from baseline (77.3% Hydrus® + CS vs 57.8% CS alone).11 The study was then continued out to 5 years of follow-up to monitor safety and efficacy outcomes; however, medication washout was not continued beyond 24 months. Data from years 3 to 5 demonstrated continued durability in the IOP response, while also providing insights into the impact that MIGS can have on the clinical course relative to CS alone. For example, the data at both 2 and 5 years of follow-up demonstrated a higher percentage of patients on zero medications, a significant reduction in the need for invasive secondary surgical intervention, and a greater-magnitude reduction in IOP in the Hydrus® + CS group compared to CS alone.11,15
In Their Own Words
How Can the Evidence From HORIZON Inform Decision-Making?

Pradeep Ramulu, MD, PhD: Every eye that has moderate or advanced glaucoma once had mild disease. That fact should guide our thinking about how we treat patients with mild primary-open angle glaucoma (POAG)—we just do not know which patients will progress and which won’t. Based on the HORIZON trial, we have evidence that intervening early has a meaningful impact on the long-term outcome: more eyes achieved medication-free status and fewer eyes required a secondary surgical intervention. Based on that, one could argue that you have an obligation to discuss minimally invasive glaucoma surgery (MIGS) options with patients who take medications for POAG and have a visually significant cataract if they are eligible for the surgery. If you don’t, there’s a chance that patient will hear about it from a friend or family member, and you suddenly have a dissatisfied patient.

I. Paul Singh, MD: The HORIZON trial showed that Hydrus® + cataract surgery is an effective IOP-lowering procedure that has a good chance of lowering patients’ reliance on medications. These data give me confidence in using the device in appropriately selected patients regardless of glaucoma stage. In my thinking, the reduced requirement for secondary interventions in the Hydrus® Microstent + cataract surgery group compared to the cataract-surgery-alone group suggests that treating the anatomy underlying the glaucomatous pathology had a meaningful effect on long-term outcomes. If you believe that to be the case, why not present it as an option for patients with POAG, regardless of whether it is mild or moderate?

Brian Flowers, MD: When we sit with our patients, the options are often presented in a binary fashion. What we have learned from HORIZON and other studies forces us to rethink whether this is the case. There is mounting evidence that MIGS offers not only pressure control, but also less medication burden long-term with procedural interventions. It is difficult to know if this is based strictly on compliance or some other factors. Nevertheless, it’s becoming difficult to ignore at this point.
Confidence in the Data
From our perspective, there are several reasons why the HORIZON data should help to shape clinical decision-making (see In Their Own Words). For instance, there is accumulating evidence to support the idea that MIGS devices have an additive, clinically meaningful effect on IOP lowering compared to CS alone. Although it is well known that CS alone lowers IOP,16 data from major clinical trials suggest that MIGS devices deliver consistently better IOP-lowering efficacy. In the COMPASS, HYDRUS II, and HORIZON trials, a MIGS device plus CS was compared to CS alone. Across the three studies, the IOP-lowering efficacy of CS alone was similar. However, in each trial, MIGS plus CS conferred a consistently greater reduction in IOP.11,12,17 Furthermore, in the HYDRUS II Study, mean diurnal washed-out IOP in the Hydrus® + CS group was slightly lower when compared to the CS alone group at 12 months, and then the IOP rebounded at 24 months in the CS alone group, suggesting greater durability with MIGS devices (Figure 2).12
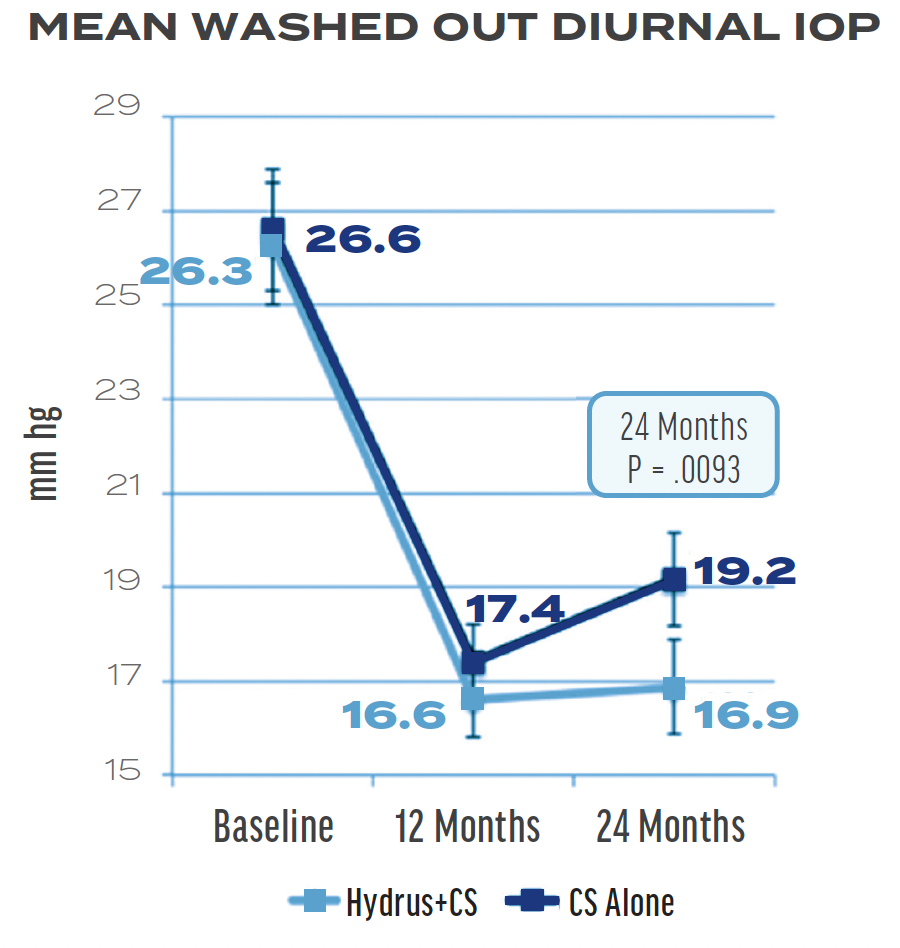
Figure 2. Graph showing the IOP response to Hydrus® + cataract surgery (CS) and CS alone in the Hydrus II study. The rebound of IOP in year 2 in the CS group suggested greater durability with the Hydrus® Microstent.12
Another reason we can feel confident in the HORIZON data is the study’s design and methodology. Conceived as a 5-year prospective study, the first 2 years of the study comprised the pivotal phase, and then patients were followed for an additional 3 years to further assess safety and efficacy. The length of prospective follow-up in HORIZON is unprecedented in terms of MIGS studies, as is its patient retention rate: the study was able to retain 80% of patients (n = 442/556) originally randomized to receive a Hydrus® Microstent through 5 years.15 Furthermore, compared to other pivotal studies which only enrolled patients from the United States, HORIZON enrolled patients from nine countries on three continents. Taken together, these facts make it more straightforward to apply the data in real-world settings as we counsel patients on their options for managing POAG.
Conclusion
The HORIZON Trial met its primary endpoint at 2 years in demonstrating a higher percentage of patients with a reduction of at least 20% in mean washed-out diurnal IOP from baseline after receiving Hydrus® + CS compared to CS alone.11 Longer-term follow-up helped to confirm the safety and efficacy of the device.14,15 These data alone are impressive in showing the benefits of a MIGS device in delivering long-term outcomes. Yet, a deeper look at the findings from HORIZON suggests that adopting a proactive mindset by intervening earlier in the disease course with Hydrus® + CS has many benefits: at both 2 and 5 years of follow-up, patients in the Hydrus® + CS arm of the HORIZON Trial were more likely to be on zero medications and were less likely to require more invasive surgical intervention.11,14,15 Furthermore, it is worth noting that Hydrus® is consistently recognized for the highest data quality among all MIGS.*18-20
Based on these learnings, we can have confidence in counseling patients regarding how the Hydrus® Microstent could decrease their medication burden. It is, indeed, the total evidence from HORIZON that supports the idea that MIGS can have a meaningful impact on patients' quality of life. These learnings can guide clinical decision-making with respect to the treatment algorithm for the patient with POAG.
*AAO: Hydrus® received a data rating of “moderate quality, strong recommendation,” the highest rating among all MIGS; Cochrane: Hydrus received the “moderate certainty” grade of evidence in an independent systematic review in 2020; EGS: Hydrus® received a data rating of “moderate,” the highest rating among all MIGS
1. Gedde SJ, Herndon LW, Brandt JD, et al; Tube Versus Trabeculectomy Study Group. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804-814.e1.
2. Gedde SJ, Feuer WJ, Lim KS, et al; Primary Tube Versus Trabeculectomy Study Group. Treatment Outcomes in the Primary Tube Versus Trabeculectomy Study after 5 Years of Follow-up. Ophthalmology. 2022;129(12):1344-1356.
3. Saheb H, Ahmed II. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23(2):96-104.
4. Yang SA, Mitchell W, Hall N, et al; IRIS® Registry Data Analytics Consortium. Trends and usage patterns of minimally invasive glaucoma surgery in the United States: IRIS® Registry Analysis 2013-2018. Ophthalmol Glaucoma. 2021;4(6):558-568.
5. Micheletti JM, Brink M, Brubaker JW, et al. Standalone interventional glaucoma: evolution from the combination-cataract paradigm. J Cataract Refract Surg. 2024;50(12):1284-1290.
6. Johnson M. What controls aqueous humour outflow resistance? Exp Eye Res. 2006;82(4):545-557.
7. Goel M, Picciani RG, Lee RK, Bhattacharya SK. Aqueous humor dynamics: a review. Open Ophthalmol J. 2010;4:52-59.
8. Battista SA, Lu Z, Hofmann S, et al. Reduction of the available area for aqueous humor outflow and increase in meshwork herniations into collector channels following acute IOP elevation in bovine eyes. Invest Ophthalmol Vis Sci. 2008;49(12):5346-5352.
9. HYDRUS® Microstent [instructions for use]. Irvine, CA: Alcon Vision LLC; September 2021 (United States).
10. Market Scope 2021 Glaucoma Surgical Device Market Report: 2020-2026. July 2021.
11. Samuelson TW, Chang DF, Marquis R, et al; HORIZON Investigators. A schlemm canal microstent for intraocular pressure reduction in primary open-angle glaucoma and cataract: The HORIZON Study. Ophthalmology. 2019;126(1):29-37.
12. Pfeiffer N, Garcia-Feijoo J, Martinez-de-la-Casa JM, et al. A randomized trial of a schlemm’s canal microstent with phacoemulsification for reducing intraocular pressure in open-angle glaucoma. Ophthalmology. 2015;122(7):1283-1293.
13. Allingham RR, de Kater AW, Ethier CR. Schlemm’s canal and primary open angle glaucoma: correlation between Schlemm’s canal dimensions and outflow facility. Exp Eye Res. 1996;62(1):101-109.
14. Ahmed IIK, Rhee DJ, Jones J, et al; HORIZON Investigators. Three-year findings of the HORIZON Trial: a schlemm canal microstent for pressure reduction in primary open-angle glaucoma and cataract. Ophthalmology. 2021;128(6):857-865.
15. Ahmed IIK, De Francesco T, Rhee D, et al; HORIZON Investigators. Long-term outcomes from the HORIZON Randomized Trial for a schlemm’s canal microstent in combination cataract and glaucoma surgery. Ophthalmology. 2022;129(7):742-751.
16. Mansberger SL, Gordon MO, Jampel H, et al; Ocular Hypertension Treatment Study Group. Reduction in intraocular pressure after cataract extraction: the Ocular Hypertension Treatment Study. Ophthalmology. 2012;119(9):1826-31.
17. Vold S, Ahmed II, Craven ER, et al; CyPass Study Group. Two-Year COMPASS Trial Results: supraciliary microstenting with phacoemulsification in patients with open-angle glaucoma and cataracts. Ophthalmology. 2016;123(10):2103-2112.
18. Gedde SJ, Vinod K, Wright MM, et al; American Academy of Ophthalmology Preferred Practice Pattern Glaucoma Panel. Primary Open-Angle Glaucoma Preferred Practice Pattern®. Ophthalmology. 2021;128(1):P71-P150.
19. Abegao Pinto L, Sunaric Mégevand G, Stalmans I, et al; EGS Surgery Taskforce. European Glaucoma Society – A guide on surgical innovation for glaucoma. Br J Ophthalmol. 2023;107(Suppl 1):1-114.
20. Otarola F, Virgili G, Shah A, et al. Ab interno trabecular bypass surgery with Schlemm´s canal microstent (Hydrus) for open angle glaucoma. Cochrane Database Syst Rev. 2020 Mar 9;3(3):CD012740.



