
Cataract and refractive surgery techniques have changed immensely in the past few years, with precision lasers and wavefront-measuring techniques providing physicians with more accuracy and a better understanding of the intricacies of the ocular surface. I always seek the greatest level of precision for every treatment; however, IOL power calculation is one area that has eluded high levels of accuracy.
I have used many of the available tools for preoperative keratometry (K) readings, including the Javal keratometer, the Pentacam (Oculus Optikergäte GmbH) coupled with the Holladay 2 formula, and the IOLMaster’s partial coherence interferometry (Carl Zeiss Meditec) for axial length measurements. The trend in my practice has been significant variation in results—in other words, different equipment providing different measurements, even for the same patient. I recently began using the Optiwave Refractive Analysis System (ORA System; WaveTec Vision) to confirm preoperative readings with intraoperative aberrometry measurements and to achieve greater control and precision in my surgeries.
Take-Home Message
- Take intraoperative measurements as precisely and quickly as possible to avoid variance in readings.
- The key elements of a correct reading are IOP between 20 and 30 mm Hg, central 4-mm clear media from cornea to retina, and an evenly moist corneal surface.
- According to data on file with WaveTec Vision, surgeons using the ORA System can achieve ±0.50 D of intended correction in 81% of cases
Talbot-Moiré interferometry can accommodate the range of refractive error observed in aphakic and pseudophakic eyes. The ORA System combines these refractive measurements with algorithms for calculating IOL measurements that have been refined using data from nearly 30,000 procedures. Using this tool, I have improved the accuracy of IOL selection and almost eliminated the occurrence of refractive surprises, even in long and short eyes.
Accurate intraoperative measurements allow the surgeon to get the correct refractive result. In comparing my readings from the IOLMaster with the Holladay 1 formula and the intraoperative readings taken with my WaveTec device, there is a discrepancy in approximately 66% of cases (personal data). I have found that the intraoperative readings are always more accurate.
PRACTICE PEARLS
Intraoperative aberrometry can be an excellent tool, but like all instruments it must be used correctly to get the most accurate output. Three key elements in a correct reading are (1) intraocular pressure (IOP) of between 20 and 30 mm Hg, (2) central 4-mm clear media from cornea to retina, and (3) an evenly moist corneal surface.
I start with generous injection of a cohesive ophthalmic viscosurgical device (OVD) into the anterior chamber through a secondary incision, until I see OVD flowing back out from the injection site. Because the eye is open and not blinking, it is necessary to continuously moisturize the eye with balanced saline solution. Continual IOP monitoring is also needed. Once all three of these elements are achieved, I quickly take my measurements. When multiple measurements are taken, the IOP can dip and the eye can get softer, making variance in the readings more likely. I find it valuable to take the measurements as precisely and quickly as possible.
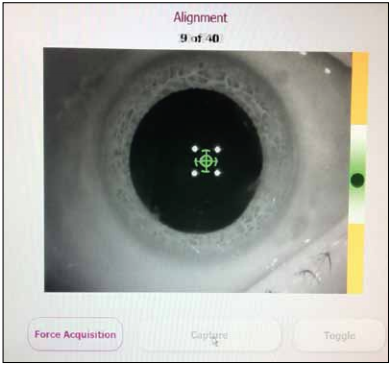
Figure 1. The optimal position to take a good intraoperative aberrometry measurement is in the green crosshairs section, at or just below center. (This image was enhanced using Photoshop.)
It is also important to ensure that the eye is aligned and centered and that the aberrometer is at a safe distance from the eye. The round, dark ball should be vertically aligned; the optimal position to take a good measurement is in the green crosshairs section, at or just below center (Figure 1). If measurements are taken in the extreme top or bottom of the green crosshairs, it is possible to have up to a 0.50 D difference in measurements.
APPLICABLE FOR ALL PATIENTS
Every eye can benefit from the additional precision of intraoperative aberrometry; however, it is especially helpful in difficult cases such as postrefractive surgery patients. For example, a patient who had undergone radial keratotomy several years ago presented with a cataract. I operated on her first eye approximately 3 months ago and achieved a spherical equivalent of approximately plano using intraoperative aberrometry to confirm my preoperative readings. I performed intraoperative aberrometry with the second eye as well; however, hyperopia was seen 2 weeks after surgery. Even with this complication, the patient is happier with the second eye than she was with the first eye at the same stage.
Achieving excellent results with lens-based vision correction requires accurate calculation of IOL power. I believe that intraoperative aberrometry is the most accurate instrument to obtain these outcomes. To support this claim, recent data from WaveTec show that surgeons using the ORA System can achieve within ±0.50 D of intended correction in 81% of cases (data on file with WaveTec Vision).
CONCLUSION
We should stop thinking of intraoperative aberrometry as an optional enhancement for our patients and start considering it a necessary tool for all patients. Intraoperative aberrometry has made my surgeries as accurate as possible, even for cataract surgery after refractive surgery. When you position your practice as a laser refractive clinic promising excellent visual acuity, it is imperative to use the tools that allow you to offer the best results possible.
Miguel A. Santiago Garcia, MD, practices in Carolina, Puerto Rico. Dr. Santiago Garcia states that he has no financial interest in the products or companies mentioned. He may be reached at e-mail: miguel.santiago@ojosypiel.com.
