

The COVID-19 crisis has severely affected the way we all practice. Most ophthalmic clinics are now seeing or just emerging from seeing only patients who require urgent care. At the time of this writing, in the United Kingdom, routine surgical procedures had been unequivocally suspended based largely on advice from the government and the Royal College of Ophthalmologists. Similarly, community-based optometry practices, based on advice from the government and the College of Optometrists, had stopped all routine eye examinations and are now performing only urgent and essential care services.
The current situation has given us all time to reflect on what professional life will be like after the lockdown is lifted. It is fair to assume that, certainly in the short term, things will not be the same. Many of us are planning for how to manage patient flow in view of the likelihood that social distancing will continue for quite some time. We are also forecasting how to make the inevitable reduction in numbers fit within our models and keep our businesses viable at the same time.
Refractive surgery centers are a potential hotbed for COVID-19 transmission and infection. We must find ways to avoid the large numbers of patients waiting to be examined, for their drops to take effect, and for their surgery. We must also find ways to decrease the number of patients and their companions resting in recovery. Therefore, protocols must be developed that minimize infection risk to both patients and staff while maintaining business continuity.
SHARED CARE
Optometrists and ophthalmologists have had symbiotic relationships for several decades. Ultimately, we are looking after the same patients, and there are many examples where collaborative arrangements have proved beneficial to both the professionals and their patients. Shared care, or comanagement, is well-established in some regions of the world, and most of these arrangements have well-defined protocols and a good business structure in place so that each party is aptly remunerated for its time and involvement.
At the other end of the scale, there are some schemes in which payment of a so-called comanagement fee is no more than a referral fee. At a time when regulators are particularly keen to avoid bribery and its appearance, such business practice is far from desirable. It is important to examine the negatives of such comanagement schemes to avoid the same issues going forward.
Previously in the United Kingdom, some schemes offered financial incentives for referral without asking for any significant pre- or postoperative involvement on the part of the optometrist. Such schemes tended to be within the domain of commercial, high-volume clinics. In some instances, protocols were developed whereby the optometrist recorded vision and had a cursory look with a slit lamp to justify payment. Such schemes, which had their peak popularity around the early 2000s, tended to be associated with laser refractive surgery.
REDUCING THE BURDEN
As a result of these negative connotations, shared care within the private sector took a resounding knockback, so that now there are few schemes in which ophthalmologists and optometrists truly work in collaboration. However, within the National Health Service, several shared-care schemes do exist. Their aim is primarily to reduce the burden on busy clinics.
For example, successful community-based schemes are already in place for diabetic shared-care, cataract postoperative care, and IOP management in glaucoma. For these schemes, the community optometrist is often trained by the hospital to be competent within the bounds of an agreed protocol. Some may also involve a formal examination to prove competence.
These schemes are useful in keeping National Health Service waiting times down, but the burdens of equipment, education, and revalidation for these programs often tend to be at an entry level to encourage widespread participation. As such, it can be questioned whether the patient is getting a real benefit or whether such schemes are useful only in maintaining numbers.
ADAPTING TO CHANGE
Community-based optometry practices are often located in convenient High Street or busy urban areas and within easy access for most patients. In the United Kingdom, a differentiating feature of such practices is whether they are owned by a group (a chain or multiple) or are independently owned. Within a multiple practice, the optometrist is often bound by criteria set by the group to maintain uniformity. This can often affect the type of equipment available and the clinical services offered. The group may also determine the clinical direction that a practice may take. Many of the individual practices within a chain are owned by franchisees, who have limited autonomy to introduce new services.
Independent practices, on the other hand, have no external limitations other than those of the governing bodies and are generally freer to purchase equipment as desired and to introduce additional services more rapidly. Such practices may afford a major advantage after the lockdown, as they will be able to adapt quickly to change.
A well-equipped optometry practice will boast an impressive panel of diagnostic equipment, and the resident optometrist will generally be well-versed in the use of these devices and the interpretation of the results obtained. In such premises, ultra-widefield scanning laser ophthalmoscopy, OCT, digital slit lamps, corneal topography, axial length measurement capabilities, and other advanced clinical technologies are not unusual.
COMMUNICATION AND COLLABORATION
These practices potentially offer an ideal environment for refractive and cataract patients to be seen pre- and postoperatively, in an environment that provides a reduced COVID-19 infection risk compared with a busy refractive clinic. To establish this type of arrangement, the parties must have a good working relationship, and protocols must be put into place that allow easy communication and safe patient care.
The optometrist must undertake appropriate training, as required, and receive adequate remuneration for time spent with the patient. The ophthalmologist should feel confident in his or her colleague’s ability and be able to provide a facility where any concerns the optometrist has can be addressed, particularly before the patient is seen in the clinic. Additionally, there should be scope for the ophthalmologist to examine a patient before any surgery, particularly if this is flagged as necessary by the optometrist. The most important factor on both sides, however, is the means to have open and frank communication so that the standard of care is never compromised versus being seen in the operating clinic alone.
Community-based comanagement can have no prescriptive structure and will vary from one optometrist-ophthalmologist relationship to the next. Before any scheme can be implemented, clear protocols and a relationship agreement should be in place. Moreover, there should be a clear plan for emergencies and after-hours care if required. A broad structure is indicated in the Figure.
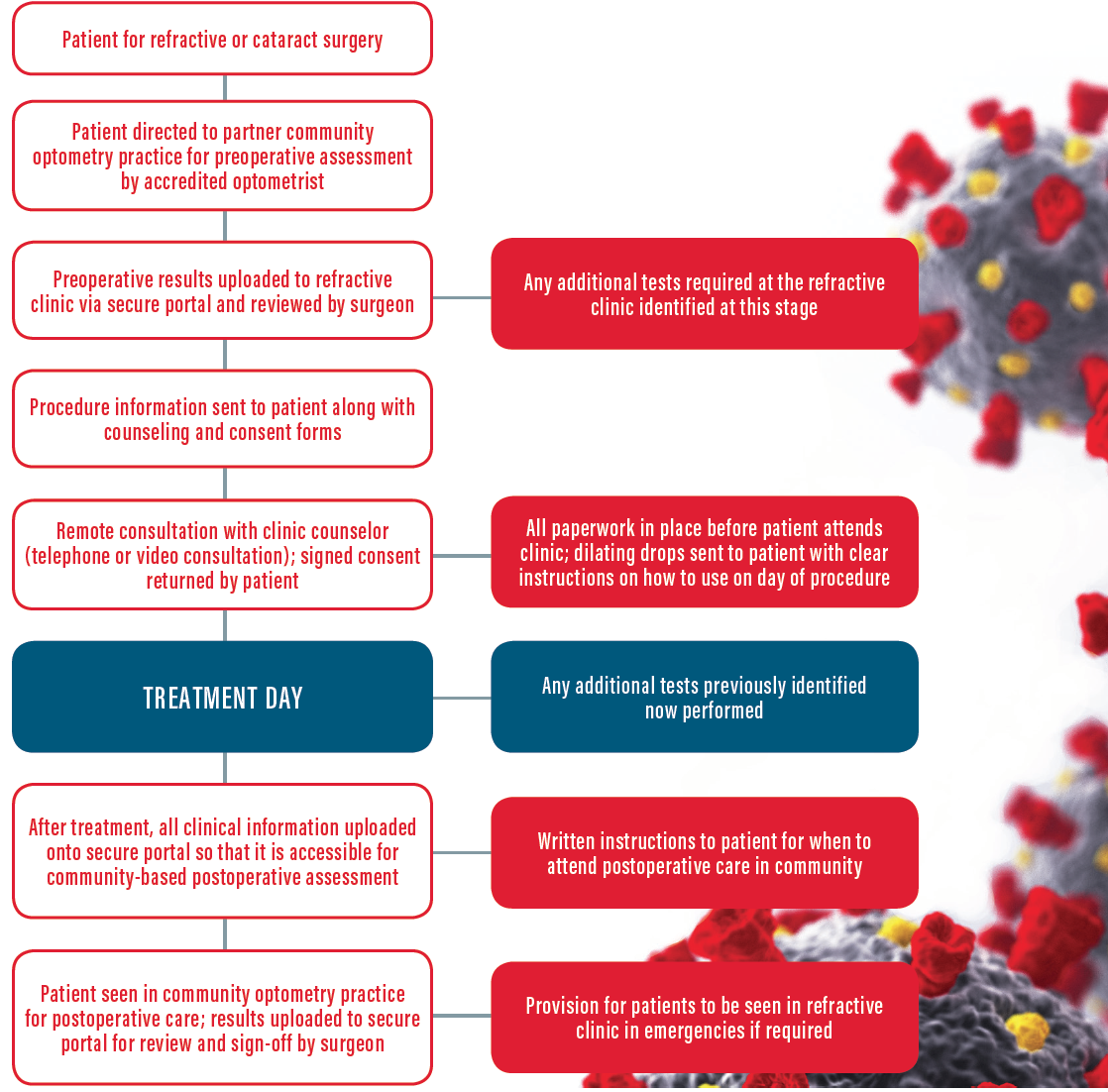
Figure. An example of a post-lockdown optometry-ophthalmology shared-care pathway.
ESTABLISHING PROTOCOLS
A shared care scheme can present certain challenges. The established protocols must acknowledge the limitations of what can be done in community-based practice, and safeguards should be put into place for unexpected outcomes so that each party is acting with the patient’s best interest in mind.
The optometrist may require upskilling before participating in comanagement, and the onus for this training should lie on the refractive clinic. A formal examination and accreditation should be considered to prove competence.
Financial arrangements should be transparent and presented to the patient before any preoperative examination. It should be clearly indicated that payment is for the clinical time and expertise in examining the patient rather than as an incentive or referral fee. This is particularly relevant when the patient undergoing treatment has been referred from the community practice’s own database.
Above all, a system must be established to allow the safe flow of clinical information between the refractive clinic and the community-based practice. Both parties must adhere strictly to the European Union’s General Data Protection Regulation requirements when patient-sensitive information is disseminated. There are several ways of creating such a system, but arguably the simplest is via a secure portal allowing ease of communication among all parties involved in the patient’s care.
PATIENT BENEFITS
There are clear and significant advantages to patients in a community-based, shared-care approach. A well-thought-out and implemented scheme can be beneficial to the community optometrist by bringing more varied work to the practice, establishing a new revenue stream, and earning kudos for being associated with a gold-standard refractive clinic. For the refractive clinic, the arrangement allows patients to be seen by skilled, community-based colleagues in an environment with a significantly reduced infection risk. It also facilitates better social distancing and patient flow once the patient is in the clinic.
The current crisis has allowed us to reflect on how we will safely practice in the future. Shared-care schemes in refractive surgery are not new. In the United Kingdom, in particular, their previous incarnations were poorly planned, resulting in such schemes being brought into disrepute. A transparent, well-implemented comanagement scheme today can significantly enhance the patient experience and reduce the risk of COVID-19 infection for patients and clinicians alike.
