
Sponsored by




Any surgical method that requires external access to the eye through the conjunctiva and sclera can lead to proliferation of fibroblasts and subsequently to the increased risk of scar tissue and loss of aqueous humor flow. In the past 10 years, interest in glaucoma surgery has increased and many new procedures have surfaced for the treatment of early- to mid-glaucoma disease. Among them is a new classification of surgical procedures described as microinvasive glaucoma surgery (MIGS). The big draw to MIGS is that it can be performed relatively quickly and minimally invasively. Additionally, many of these procedures have had promising results with respect to reduction of IOP and their low risk of complications.1-3
One procedure in the MIGS category is High Frequency Deep Sclerotomy (HFDS).* Developed by Bojan Pajic, MD, PhD, FEBO, at the Eye Clinic ORASIS in Switzerland, this ab-interno method is based on making six small pockets through the trabecular meshwork and Schlemm canal and into the sclera. The bipolar abee probe (Oertli Instrumente AG; Figure 1) is used to create these elliptical pockets by spreading heat and high-frequency energy around the tip, resulting in highly focused heating of the tissue.
Figure 1. The bipolar abee probe creates elliptical pockets by spreading heat and high-frequency energy around the tip.
The HFDS procedure is completed in eight simple steps, which are illustrated on the following page. We started using HFDS in the spring of 2016 and, as far as we know, we were the first practice in Scandinavia to perform the method for the treatment of glaucoma. Fifty patients who originally have been referred for filtration operations have successfully been treated with HFDS so far. The procedure takes only a few minutes and can be performed as a standalone procedure or in combination with cataract surgery.
six key advantages
Our experience with HFDS has been positive, and we have identified six key advantages:
- 1. No bleb-related filtration complications;
- 2. No impact on refractive power;
- 3. No scar tissue in the sclera around the pocket;
- 4. Absence of foreign body/implant/shunt postoperatively;
- 5. Repeatable if necessary; and
- 6. Simple and time- and cost-effective (reusable probe).
Eight Steps of the HFDS Procedure
Step No. 1: Inject intracameral carbahol/myochol for pupil constriction.
Step No. 2: Fill the anterior chamber with a visoelastic device.
Step No. 3: Apply methocel on the cornea.
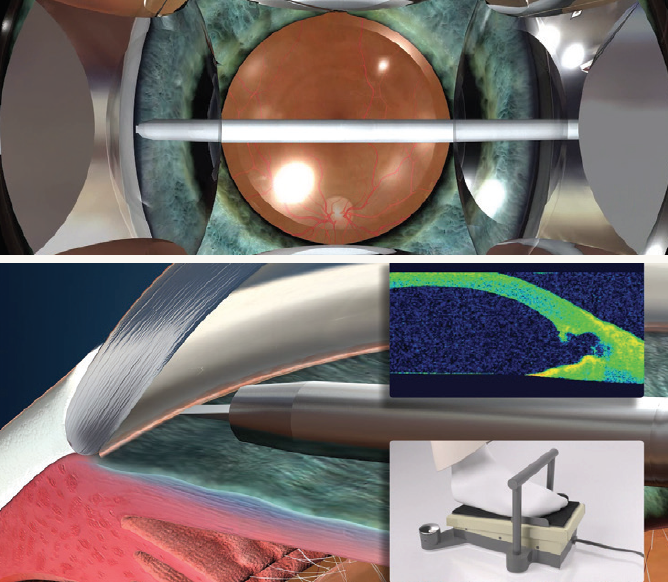
Step No. 4: Insert the abee probe into the anterior chamber through a temporal paracentesis or the main incision. The probe should penetrate the trabecular meshwork on the nasal side.

Step No. 5: Place the gonioscopy lens (direct or indirect four-mirror) on the cornea to visualize the iridocorneal angle.
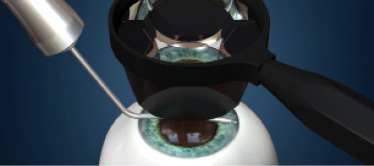
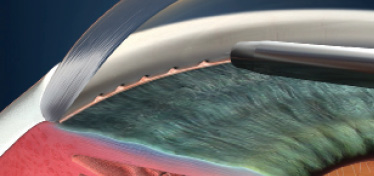
Step No. 6: Place the tip against the trabecular meshwork; press the footpedal and move the tip forward at the same time to penetrate the trabecular meshwork. With bipolar diathermy, a pocket that is 0.3 mm high, 0.6 mm broad, and 1 mm deep is performed.
Step No. 7: Pull the abee tip backward.
Step No. 8: Repeat the procedure five times until there are six pockets.
CONCLUSION
In our experience, HFDS is an effective, minimally invasive, and safe procedure for the treatment of patients with primary open-angle glaucoma. HFDS is a good choice for patients with mild to moderate glaucoma, optionally in combination with cataract surgery; juvenile glaucoma; regulated glaucoma, to reduce the use of IOP-reducing drops or when poor compliance is suspected; younger patients; and contact lens users. We believe the method will be widely used in the future both in- and outside Nordic countries.
1. Pallas G, Pajic B. Die Sklerathalamektomie (STE): Stabile postoperative Augendruckregulierung beim Offenwinkel- und Kapselhäutchenglaukom. [In German.] Klein Monatsbl Augenheilk. 2000;216:256-260.
2. Pajic B, Pallas G, Gerding H, Böhnke M. A novel technique of ab interno glaucoma surgery: Follow-up results after 24 months. Graefes Arch Clin Exp Opthalmol. 2005;19:1-6.
3. Pajic B. High-Frequency Deep Sclerotomy. Cataract & Refractive Surgery Today. October 2011.
*HFDS is not available for sale in the United States.
HFDS and abee are registered trademarks of Oertli Instrumente AG, Switzerland.
© 2017 Oertli. All other brand/product names are the trademarks of their respective owners.


