



For a novice, cataract surgery on an eye with pseudoexfoliation (PXF) syndrome may look like a nightmare. Preparing well before surgery, taking the right precautions, and following the guidelines set forth in this article can help you perform these surgeries effectively.
FIRST STEPS: SURGICAL PLANNING
The key to the proper management of PXF syndrome begins during the preoperative examination. Document signs of zonular weakening, PXF material on the anterior capsule of the cataract, elevated IOP, and a floppy iris that renders pupillary dilation difficult.
It is a good idea to watch videos of similar cases on the day before surgery. Some educational resources include Eyetube.net, Cataract Coach, and YouTube. These websites house collections of amazing videos with tips and tricks about all the complications that you may encounter during cataract surgery.
IN THE OR
I always have a pupil expander and iris hooks on hand in the OR for these cases. I also prefer to have a three-piece IOL ready for use in eyes with PXF. The pupil expander maintains optimal dilation throughout surgery. Iris hooks can be used to keep the capsular bag in place—a crucial step if you don’t trust the zonular support in one or more areas. Lastly, I like to use a three-piece IOL whenever I choose to place the IOL in the sulcus and capture the optic in the capsulorhexis and whenever I have to fixate the lens to the sclera with the Yamane technique.
Another thing to keep in mind is that PXF material can clog the trabecular meshwork and cause elevated IOP. In many instances, patients may need IOP-lowering medication preoperatively.
KEY STEPS
Scan the QR code now to watch a procedure I performed in an eye with PXF syndrome. The key steps to successful cataract surgery in eyes with PXF syndrome are outlined herein.
No. 1: Make a large capsulorhexis. A capsulorhexis of 5.5 to 6.0 mm (Figure 1) can simplify the extraction of nuclear pieces from the capsular bag. I like to perform the capsulorhexis with the anterior chamber maintainer slightly open. This helps to maintain anterior chamber pressure during this step of the procedure.
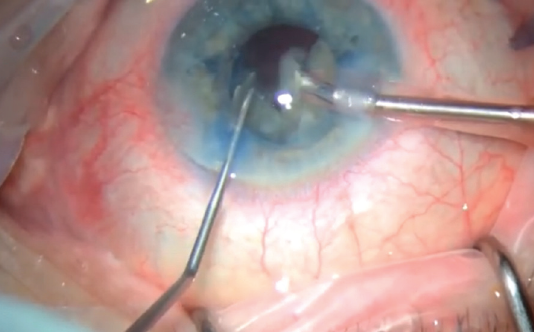
Figure 1. An appropriately sized capsulorhexis.
No. 2: Achieve adequate hydrodissection. An effective hydrodissection technique (Figure 2) will help the nucleus to rotate freely and prevent further damage to the already weakened zonules.
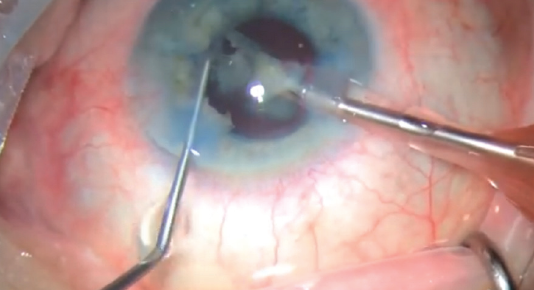
Figure 2. Thorough hydrodissection is necessary to prevent further damage to the zonules.
No. 3: Never press on the nucleus. The easiest way to tear the posterior capsule is to press on the nucleus. This movement can also compromise the capsular bag and further erode zonular support (Figure 3).
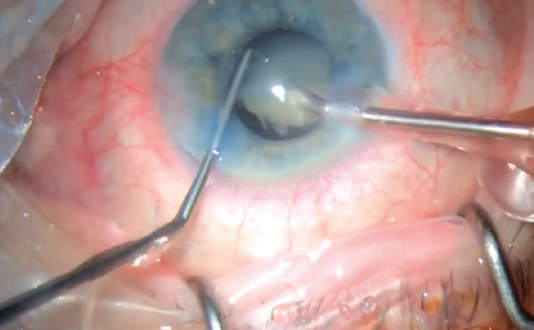
Figure 3. Pressing on the nucleus should be avoided, especially during sculpting.
No. 4: Watch the posterior capsule to prevent unnecessary fluctuations. During phacoemulsification, try to place a piece of nucleus between the posterior chamber and the piece of nucleus that is being emulsified (Figure 4).
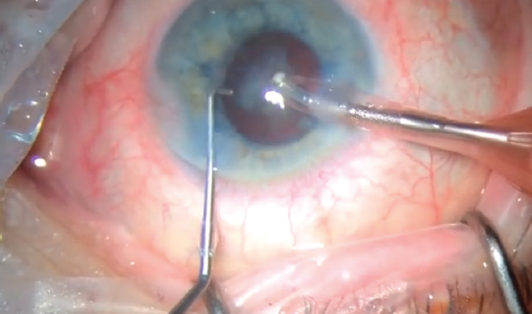
Figure 4. When the last piece of nucleus is emulsified, the chopper is placed in front of the phaco tip to protect the posterior capsule.
No. 5: Implant the IOL under irrigation. Irrigation fluid is an adequate source for maintaining anterior chamber and capsular bag stability during IOL implantation (Figure 5).
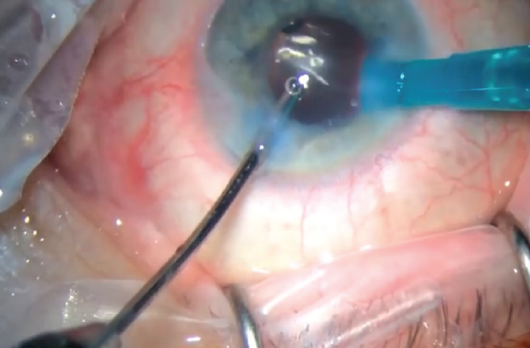
Figure 5. An IOL is implanted under the irrigation.
No. 6: Irrigate the anterior chamber angle at the end of the surgery. Irrigating the angle will mobilize the PXF material and OVD from the trabecular meshwork and keep the IOP in check postoperatively (Figure 6). Further, gently pushing down on the iris will break the anterior synechiae.
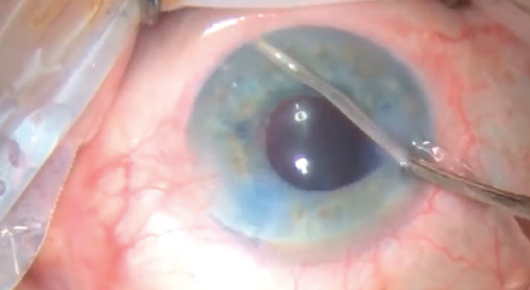
Figure 6. The angle is irrigated, and gentle pressure is applied to the iris to break the anterior synechiae.
CONCLUSION
With a steady head and a straightforward surgical technique, cataract surgery on eyes with PXF syndrome can resemble standard surgery.
