

It is no secret that today, in order to achieve the most precise outcomes in refractive surgery, the preferable method of flap creation is with a femtosecond laser. Taking this one step further, selecting the proper treatment for the individual patient and executing precise surgery are other key indicators of a successful procedure.
Below I demonstrate the advantages of using two lasers, the Victus femtosecond laser and the Technolas Teneo 317 excimer laser (both by Technolas Perfect Vision, a Bausch + Lomb company), in a refractive surgery case that required outside-the-box thinking.
CASE PRESENTATION
A 48-year-old woman with 4.50 D cylinder in her right eye (Figure 1A) and 1.00 D sphere in her left (Figure 1B) presented for refractive surgery in August 2016. The patient’s right eye was sub-amblyopic, with 0.2 logMAR BCVA. Having required spectacles for her entire life, she was now also facing symptoms of presbyopia. After discussing the surgical options with her, we decided it was best to perform LASIK in her right eye and Supracor in her left to improve both distance and near vision. As I explained, this combination would allow her to achieve unaided vision for distance, while some optical correction could be required for near vision.
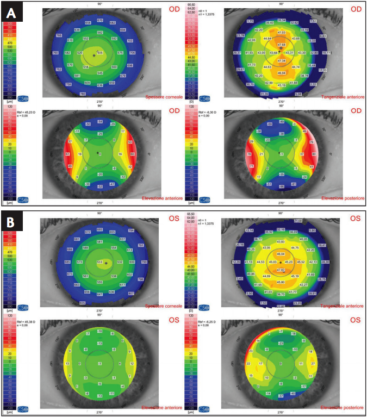
Figure 1. Right (A) and left (B) eyes preoperatively.
Flap creation. I created both flaps with the Victus femtosecond laser. I like this laser for several reasons, the most attractive of which is the ability to double-follow the corneal dissection, both from above with the embedded camera and from the side with the laser’s swept-source OCT. In this particular case, the spacing of the laser shots and the laser energy were reduced from the standard 750 nJ/5.8 μm to 700 nJ/6.2 μm because the patient did not wear contact lenses and was almost 50 years old.
LASIK treatment.I no longer mark the cornea, as this is unnecessary with the femtosecond laser. One trick to easily opening the flap and to achieving a seamless iris registration with the Teneo is to partly open the sidecut of the flap and remove the air bubbles created by the femtosecond laser. This allows me to properly engage the Teneo’s eyetracker with iris recognition before dissecting the flap, which is achieved not only precisely but also quickly.
After folding the flap back with a Seibel Lasik elevator (MMSU 1172; Malosa Medical), I prepared the eye for the treatment. I find it useful to first dry the conjunctiva. Then, with the laser compensating for every eye movement, the ablation was performed. The new plume evacuator of the Teneo 317 contains eight nozzles that are distributed homogenously over 270º. This design ensures that controlled aspiration is achieved and that a uniform laser beam is delivered throughout the duration of the ablation. Furthermore, in my opinion, the plume evacuator also clears the operating field, which is extremely helpful for patients, especially those who are anxious or nervous about undergoing surgery.
Once the ablation was achieved, I checked the status of the flap and repositioned it with irrigation. After I dried and re-wet the conjunctiva, I applied downward pressure to the flap to make sure that it was perfectly adherent to the cornea.
Supracor treatment. Supracor is a LASIK procedure for presbyopes, available on the Teneo 317 excimer laser. A small central steepening of the cornea is created to provide the wanted near addition. Again, with irrigation, I squeezed away the air bubbles via the small opening of the flap sidecut in order to engage the eyetracker. Then, I activated the iris recognition via the the graphical user interface. For this, the patient’s iris reference data was preloaded from the Zyoptix Diagnostic workstation (Technolas Perfect Vision, a Bausch + Lomb company). I then opened the flap. Another useful tip for this step is to take your time, lifting the flap in several steps in order to decrease the stress exerted on the flap and on the cornea. I have found this to be especially effective with flaps created in patients under 30 years of age.
Once the eyetracker was engaged, I performed the ablation. I referenced the Purkinje images during both fixation and the treatment to ensure that the ablation was perfectly centered.
On postoperative day 1, the patient was already satisfied with her results. The refraction in her right eye improved from 4.50 D to -0.50 D of astigmatism and UCVA from 1.0 to 0.16 logMAR (Figure 2A). As intended, in the patient’s left eye, the Supracor treatment produced a small central near add (Figure 2B). The patient achieved 0.00 logMAR UCVA for distance and for near and, even though the Supracor procedure was performed in only one eye, she was completely spectacle independent also for near vision. Over the following weeks, the result was maintained. Several years later, she is still completely spectacle independent.
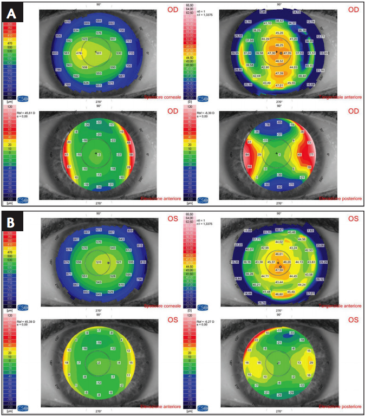
Figure 2. Right (A) and left (B) eyes 2 months postoperatively.
TOP THREE ADVANTAGES: VICTUS AND TENEO 317
In my experience, the top three advantages of the Victus are:
No. 1: Docking is easy because of the fixed two-piece curved patient interface. In corneal applications like LASIK, the Victus docks with full contact to minimize the possibility of eye tilt or distortion, meaning that precise alignment is achieved every time and also that the natural shape of the eye is maintained better than on a fully applanating system. Alternatively, in cataract surgery applications, soft docking is maintained by a thin liquid layer separating the cornea from the curved interface, thus avoiding corneal folds.
No. 2: The treatment zone can be established depending on the patient’s anatomy. In the case described herein, the treatment was centered in the middle of the suction ring; however, when some eye tilt develops at docking, the laser is still able to start working on one side of the cornea, compensating for the decentration, in order to finish treatment.
No. 3: The energy is perfectly focused. With the Victus, the applied energy is perfectly focused at a steady distance of 110 μm from the curved patient interface. The laser incorporates a specific device that varies the focal length during treatment progression in order to increase precision and decrease the total energy required.
In my experience, the top three advantages of the Teneo 317 are:
No. 1: The laser’s SyperSync ensures that the scanner, eye tracker, and laser are perfectly matched. As a result, I can be confident that all aspects of the laser will perform seamlessly.
No. 2: The new-generation ACE Eyetracker incorporates a coaxial camera (Figure 3). The incorporation of a sophisticated, multidimensional eyetracker helps me to achieve low treatment rates.
Figure 3. The ACE Eyetracker with coaxial camera.
No. 3: The laser produces a smooth ablation, thanks to its new spot distribution pattern. Instead of using a treatment card to control the shape of the truncated Gaussian laser beam, now an optical element inside the laser arm of the Teneo 317 creates the shape. Furthermore, the updated laser pattern, with a low energy soft spot of 1 mm that overlaps once every 16 pulses, minimizes the thermal effect of the laser.
CONCLUSION
The precision of the Victus and of the Teneo is unparalleled. In my practice, I now perform all standard LASIK treatments with the Victus for flap creation and the Teneo 317 for ablation. Results to date have been excellent, and patient satisfaction has remained high.
I am continually impressed by how fast this procedure is in my own clinical practice. And, as compared with other lasers, I choose the combination of the Victus and the Teneo 317 because of its accuracy in terms of the correction it performs.



