

Long-term glaucoma control increasingly requires interventions that are not only effective and safe, but economically sustainable. Among the MIGS now available, excimer laser trabeculostomy (ELIOS,* Bausch + Lomb) has emerged as a promising procedure, both clinically and, as our recent work shows, cost-effectively. In collaboration with colleagues across three continents, I participated in a systematic review, meta-analysis, and comprehensive cost-effectiveness evaluation of ELIOS. Our goal was to determine whether adding ELIOS to cataract surgery can reduce long-term economic and clinical burdens for patients and health care systems in Germany, Spain, and the United Kingdom. Importantly, our analysis demonstrated that ELIOS is a dominant strategy—delivering better clinical outcomes at lower lifetime cost—across all three health systems.
The Mechanism and Rationale for ELIOS
ELIOS is a minimally invasive laser procedure performed ab interno, either at the time of phacoemulsification or as a standalone intervention. It creates 10 precise, 210-µm micro-channels spaced across the nasal trabecular meshwork (TM), which provide direct access of aqueous humor to Schlemm's canal. By enabling physiologic outflow via these new pathways while preserving the surrounding tissues through a nonthermal photoablation process, IOP is lowered.
Unlike thermal or mechanically disruptive procedures, the excimer laser performs photoablative tissue decomposition, sparing collateral structures and maintaining the integrity of the TM. This nonthermal, tissue-preserving action is one of the reasons ELIOS retains an excellent safety profile, even compared with other MIGS options.1
Long-term evidence from university hospitals in Germany demonstrates that these microchannels remain patent for many years, supporting sustained IOP reduction.1 This duration of efficacy, combined with intuitive technique and minimal complication rates, makes ELIOS one of the most straightforward angle-based procedures for surgeons.
Systematic Review and Meta-Analysis: Efficacy and Safety
Our team conducted a systematic literature review with a meta-analysis focused on studies that reported IOP and medication outcomes after ELIOS was performed in conjunction with cataract surgery.2 From an initial pool of 90 references identified in PubMed and Embase searches, we narrowed the dataset to 17 studies that met our inclusion criteria and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Efficacy Findings
Across the included studies, patients who underwent combined ELIOS plus phacoemulsification consistently demonstrated (1) clinically meaningful reductions in IOP at 2 years; (2) a decrease in glaucoma medication use, or maintenance of the same medication burden at a lower IOP; and (3) reliable IOP reduction, even when medications remained unchanged, demonstrating the intrinsic pressure-lowering ability of the procedure itself.
The procedure’s dual capacity to reduce IOP and/or to decrease medication reliance gives clinicians significant flexibility to tailor the treatment to individual patients’ needs.
Safety Profile
ELIOS enjoys robust evidence for an excellent safety profile from thousands of treated eyes.3 In our analysis, we observed very few intra- or postoperative complications; the most common event was transient IOP elevation shortly after surgery, typically mild and self-limited. There were no significant adverse events such as persistent inflammation, hyphema requiring intervention, or damage to adjacent tissues.2
The precision and nonthermal action of the excimer laser likely contribute to this safety margin. Compared with other angle procedures, ELIOS avoids direct structural disruption of the collector system and canal wall and, with limited inflammation, is thought to induce minimal collateral damage.
Cost-Effectiveness Analysis: Model and Approach
Recognizing the need to understand the economic implications of adding ELIOS to cataract surgery, we developed a semi-Markov model, simulating disease progression across five glaucoma health states (from mild disease through severe glaucoma) with corresponding costs, medication use, and quality-of-life implications.
The model compared cataract surgery alone, which itself can provide modest IOP lowering, versus cataract surgery combined with ELIOS.
We applied: (1) data from our meta-analysis; (2) published studies on ELIOS efficacy and safety; (3) local cost weights for each country (Germany, Spain, and the United Kingdom); and (4) standard economic methods for calculating quality-adjusted life years (QALYs). Crucially, the analysis accounted for lifetime downstream costs, such as increasing medication burden, additional clinic visits, secondary glaucoma surgeries, and progression to costly advanced disease management.
Notably, the purchase cost of the excimer laser device itself was not included, as the capital equipment is typically provided on loan, with only the single-use ELIOS probe incurring a per-procedure charge.
Initial Treatment Costs: A Small Upfront Difference
ELIOS adds a modest incremental cost when paired with phacoemulsification (Figure 1), with variation driven by procedural billing structures across the three countries. These differences reflect national reimbursement structures rather than differences in the procedure itself. In Germany and Spain, bundled reimbursement means that adding ELIOS changes the total cost very little; the United Kingdom, by contrast, has more distinct billing categories. Despite this variation, the incremental upfront cost is overcome by the long-term savings generated by ELIOS’s effect on slowing glaucoma progression.
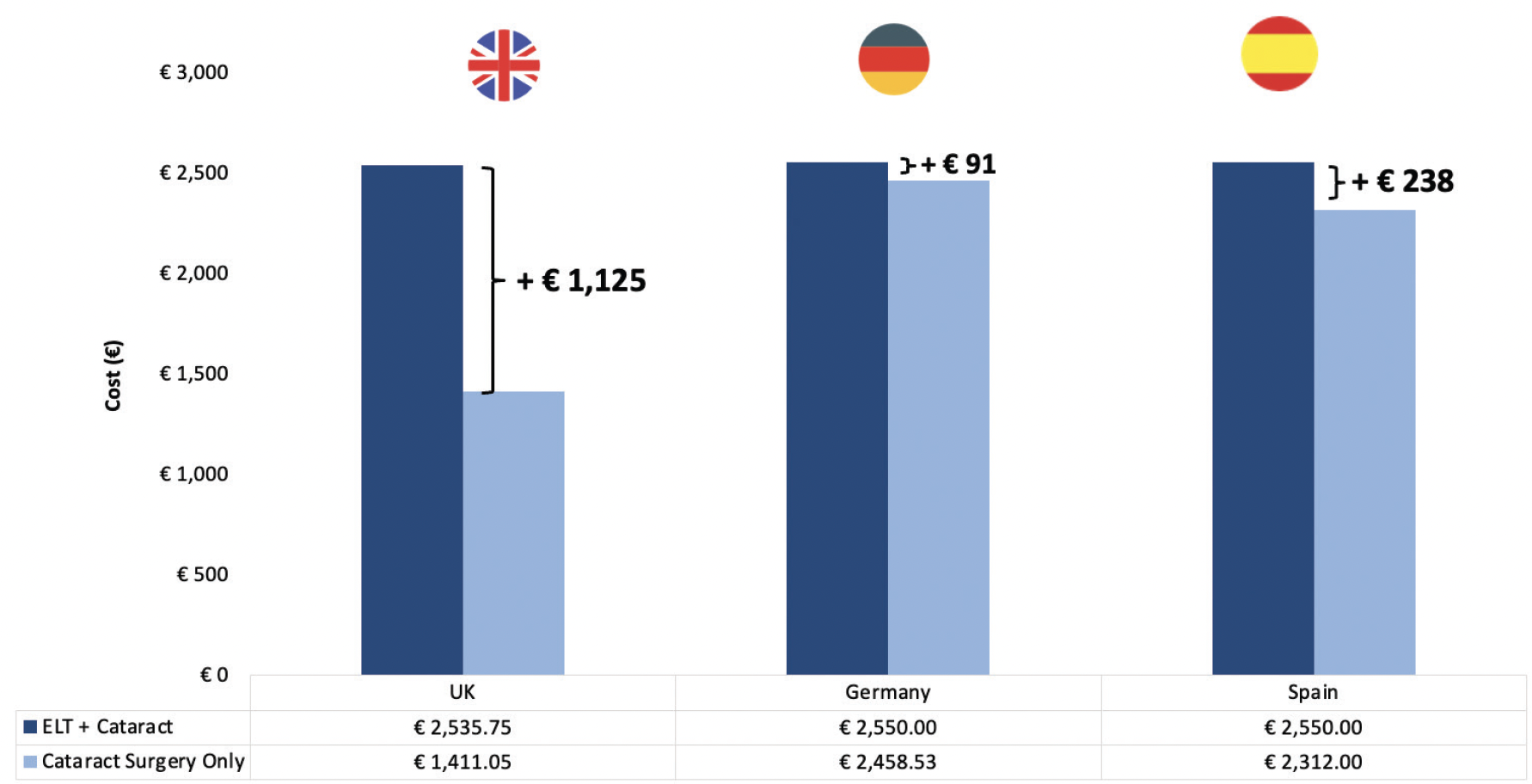
Figure 1. As expected, the initial cost of treatment is higher across all countries, although it is a one-time cost. We used local cost weights for each respective country. For the United Kingdom, we converted pounds to Euros using contemporaneous exchange rates at the time of analysis.
Lifetime Downstream Direct Medical Cost Savings
Modeling lifetime downstream costs, ELIOS emerged not only as cost-effective but as a dominant strategy, meaning it is both less expensive and more effective than cataract surgery alone (Figure 2). These findings are driven primarily by lower medication costs over time, a reduced need for secondary glaucoma surgeries, slower disease progression and fewer associated health care visits, and decreased transition into advanced, high-cost glaucoma states. In every country studied, lifetime savings exceeded the initial procedural cost, supporting the widespread adoption of ELIOS among appropriate patient groups.
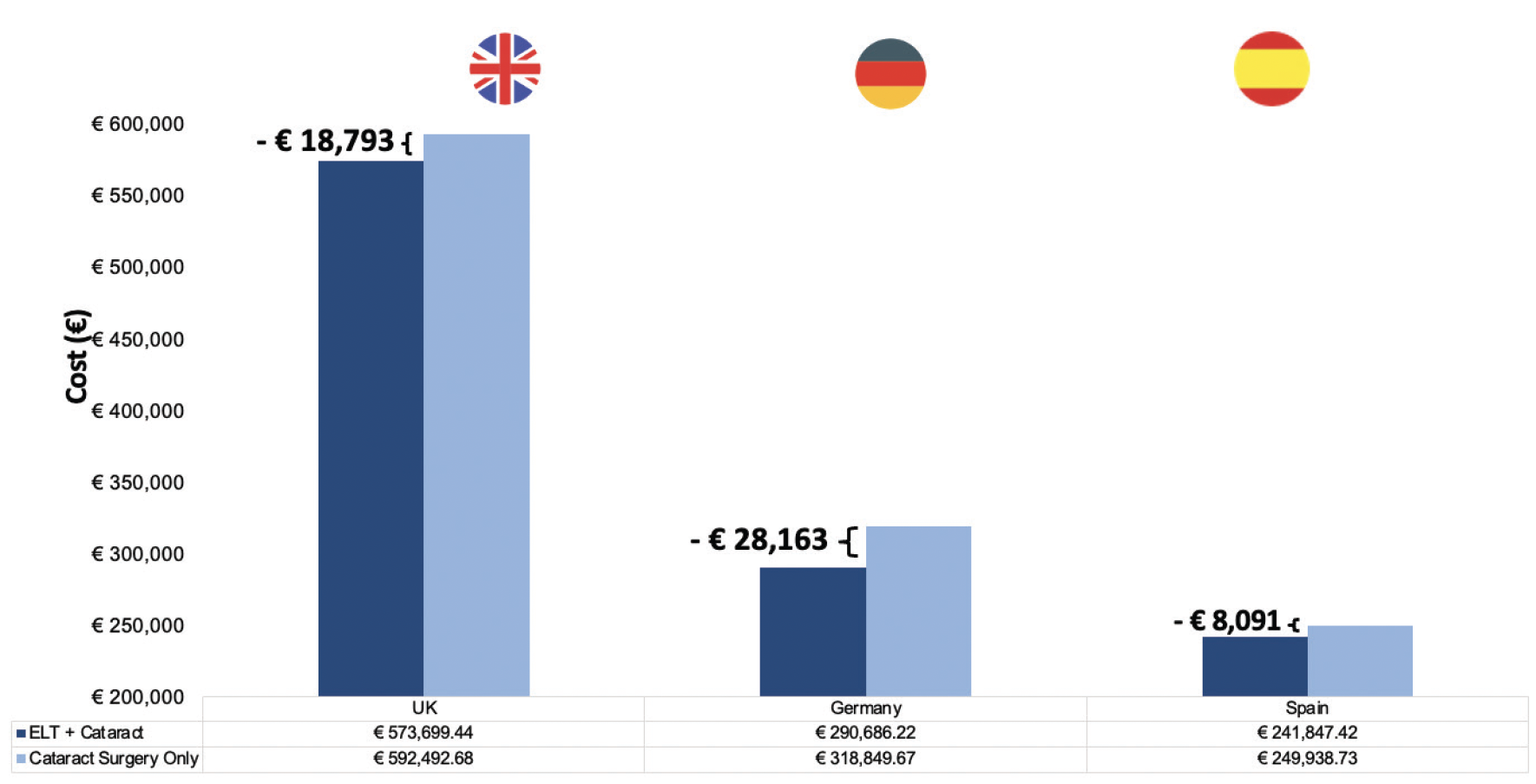
Figure 2. Across the three countries, lifetime downstream direct medical costs are greater than the initial investment. The three largest savings came from reduced trabeculectomy (and other drainage surgery) rates, routine blindness/severe POAG care, and pharmacy costs.
Quality-Adjusted Life Years (QALYs)
While differences in quality-adjusted life years were small—as expected, given that central visual acuity remains largely preserved until late-stage glaucoma—the model demonstrated a consistent QALY advantage for ELIOS (Figure 3). Even modest QALY gains reinforce the clinical meaningfulness of slowing glaucomatous progression and reducing treatment burden. Because ELIOS proved superior both clinically and in cost savings, we did not report an incremental cost-effectiveness ratio (ICER); instead, ELIOS met the definition of economic dominance in all three countries evaluated.
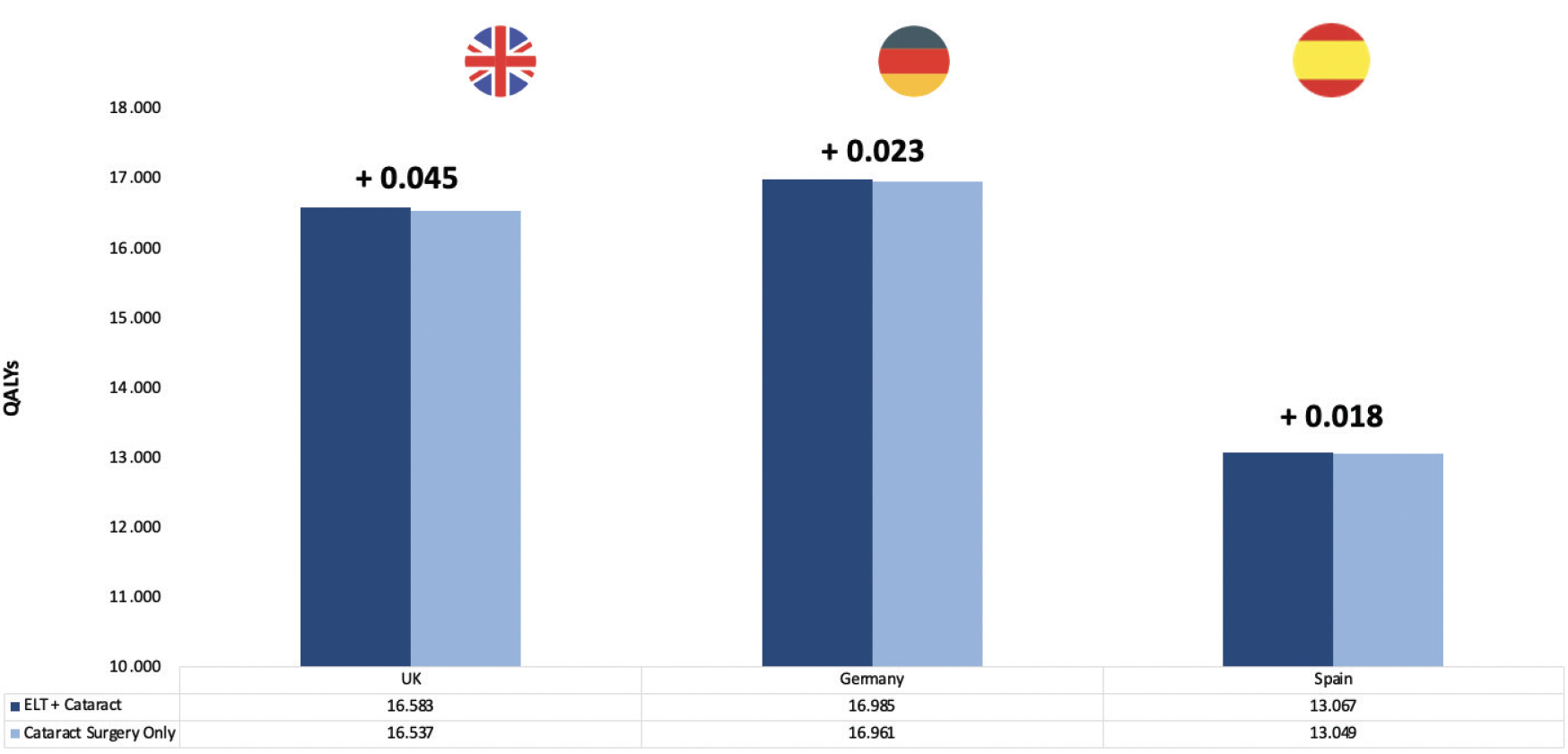
Figure 3. Across the three countries, ELIOS + cataract increased the number of QALYs over a lifetime compared to cataract surgery performed alone. (Notably, we assumed cataract surgery has no downstream adverse events, which could potentially increase the difference by 20%–30%).
Clinical Implications and Patient Selection
Although the randomized trial underlying our analysis focused on a somewhat narrower population, ELIOS is broadly applicable to patients with POAG who are already on IOP-lowering medications, individuals with mild-to-moderate glaucoma undergoing cataract surgery, and those for whom safety is a principal concern. Compared with other MIGS procedures, ELIOS offers similar safety margins relative to goniotomy or canaloplasty,1 comparable efficacy to trabecular bypass stents, and a unique advantage of nonthermal, tissue-preserving action. For patients, this translates into fewer medications, fewer surgeries, and slower progression of a life-altering disease. My colleagues and I concluded that ELIOS combined with cataract surgery offers a favorable balance of safety, efficacy, and long-term economic value across diverse health systems.
*Excimer laser trabeculostomy (ELIOS) is not available in the United States.
For more information, please visit: https://eliosvision.com/ous/
1. Berlin MS, Shakibkhau J, Tilakaratna N, et al. Eight-year follow-up of excimer laser trabeculostomy alone and combined with phacoemulsification in patients with open-angle glaucoma. J Cataract Refract Surg. 2022; 48:838–843.
2. Gazzard G, Toeteberg-Harms M, Ahmed IIK, et al. A cost-effectiveness analysis of excimer laser trabeculostomy in patients with primary open angle glaucoma in the United Kingdom, Germany and Spain. Presented at: The 43rd Congress of the ESCRS. 12-16 September, 2025, Copenhagen, Denmark.
3. Nguyen A, Simon B, Doan R, et al. Advances in excimer laser trabeculostomy within the landscape of minimally-invasive glaucoma surgery. J Clin Med. 2022;11(12):3492.
©2026 Bausch + Lomb ELS.0007
