

In the mid-1990s, the first multifocal IOLs were introduced to the market. These lenses offered patients a new opportunity for spectacle independence but sometimes at the tradeoff of visual disturbances and dysphotopsia. Most current models of presbyopia-correcting IOLs have noticeably fewer negative side effects compared to earlier generations of the lenses.
I have positive experience with many of Rayner’s IOLs, including the RayOne EMV. I am one of the first surgeons from the Sanoptis Group to implant this lens. Sanoptis has more than 200 clinics across Germany and Switzerland. In the past 6 months, I have implanted the RayOne EMV in more than 146 eyes with superb results. My patients have excellent binocular distance vision and great intermediate and near vision for most daily tasks without the need for spectacles. I am currently preparing the outcomes data for publishing.
Three tiers
As I see it, there are three tiers of presbyopia-correcting IOL solutions from Rayner, all of which have advantages and potential drawbacks (Figure).
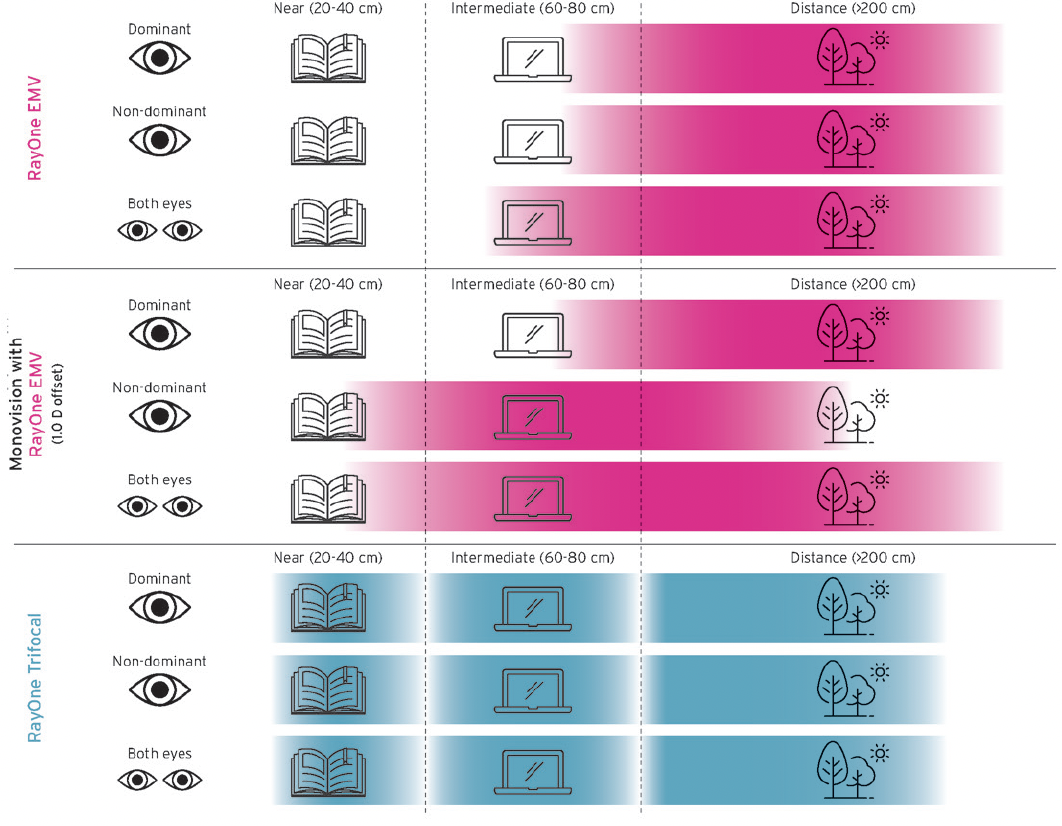
Figure. An illustration of the vision patients can expect to achieve after surgery with the RayOne EMV
and Trifocal IOLs.
Courtesy of Rayner
No. 1: RayOne EMV targeted for emmetropia. The biggest advantage of this solution is that binocular distance vision is comparable to a standard monofocal IOL but with superior intermediate vision. Patients are likely to achieve spectacle independence for intermediate distance; however, the chances for spectacle independent near vision could be lower compared to trifocal IOLs for reading small print.
No. 2: RayOne EMV targeted for monovision. The main advantage is an increase in the depth of focus compared to that of an emmetropic target in both eyes. However, patients should not be promised to achieve complete spectacle independence at all distances.
No. 3: RayOne Trifocal. Most patients like that this diffractive trifocal IOL can provide complete spectacle independence. Because of the diffractive optic, however, they may experience some dysphotopsia at night, such as halos and glare, even if they may not be considered disturbing with the latest generation of trifocal lenses.
patient education
We describe monovision in general terms, educate patients on all the available IOLs and their associated advantages and disadvantages, and share our specific approach for selecting the refractive target. We distinguish the differences between diffractive trifocal IOLs and the popular new category of enhanced monofocal IOLs, which can be used with and without a monovision strategy. We tell patients that no matter what IOL they select, there will be some compromise in their visual potential. Ensuring they understand the differences between the IOLs helps them make an educated choice based on their personal needs. I have also found that sharing my thoughts can help patients feel more confident in their decision. Lately, I tell my patients: “If I had cataracts now, I would choose the RayOne EMV IOL for my own eyes.”

IDEAL PATIENTS
My preoperative examination includes endothelial cell density measurement, OCT of the macula, and OCT angiography. Ideal patients for the RayOne EMV have no ocular comorbidities and natural levels of spherical aberration within a normal range. In my experience, the RayOne EMV is safe for eyes with mild glaucoma and for patients with diabetes if there is no evidence of retinal changes such as proliferative diabetic retinopathy. For patients with macular degeneration, there is a small risk of disease progression, but an improvement in vision and reading is possible. Such patients should understand that the potential for spectacle independence is not as it would be in a healthy eye.
Rather than always targeting plano in the dominant eye and a negative refraction in the nondominant eye, we base our decision on optical biometry results. For a monovision strategy with the RayOne EMV, I target the dominant eye for plano (range, 0.15 to -0.40 D) if the axial length difference is less than 0.2 mm. If one eye is more myopic than the other, however, the myopic eye is targeted for -0.75 to -1.00 D and the second eye is targeted for plano.
CONCLUSION
For those who want to expand their IOL offerings to include premium IOLs, the RayOne EMV enhanced monofocal is an easy entry.




{kind=link}