
Introduction
The visible spectrum is typically described as ranging from 380-720 nm. The spectral range from 380-420 nm is described as high-energy visible light. “Blue” light is the section of the spectrum that encompasses the entire bottom third of the visible spectrum from 400-500 nm.
Light shorter than 400 nm is energetic enough to cause photochemical damage to the retina but is largely screened by the cornea and natural crystalline lens.1 Light from 400-500 nm, however, can reach the retina (particularly in eyes with a UV only intraocular implant, IOL) and is energetic enough to be a catalyst for oxidative stress, particularly in elderly retinas/RPEs filled with photosensitizers.2,3 Hence, this region of the spectrum is often referred to as the “blue light hazard”.4
Intraocular filters
The human cornea absorbs all the UV radiation below 295 nm and the natural crystalline lens absorbs most light near UV-B (300-315 nm);1 the absorption of short-wavelength visible light is augmented with age.5 The human crystalline lens is only clear at the very beginning of life, the UV-light absorption by the natural lens leads to the photo-oxidative processes in the lens, which results in the formation of yellow-brown pigments.6,7 Due to changes in the lens with age, the cataractous lens absorbs more of the shorter-wavelength light, which further limits the amount of short-wavelength light (300-400 nm) propagated to the retina.7
Given the prevalence of blue light filters (BLF) in the natural world, it is not surprising that many IOL designs mimic this strategy. However, not all IOL filters are the same. Figure 1 shows the transmission characteristics of several BLF and non-BLF IOLs currently on the market. The AcrySof UV IOL (Alcon) only absorbs light in the ultraviolet spectrum. The TECNIS Symfony OptiBlue filter primarily absorbs in the UV and violet spectrum (Johnson & Johnson Vision; IOL DFU[IA1] ). The AcrySof Natural and Clareon IOLs (both from Alcon) have nearly identical UV and BLF absorption, which were designed to match the spectrum of the human crystalline lens of a healthy adult, particularly in the 400-475 nm range.8
Equivalence between AcrySof IQ Natural IOL and Clareon
As with many other technologies, one popular strategy has been to replace an elderly cataractous lens with an implant that matches the spectral, and many of the optical, features of the young natural adult lens.8 This is contrasted with implants that are perfectly transparent to visible light. Two popular BLF IOLs are the Acrysof IQ Natural and the Clareon. These lenses utilize the same chromophore to produce a similar absorbance profile as shown in Figure 1. The two lens types share many features (haptic design, spherical aberration profile, and optical zone diameter) but are different in some other categories. These include a modified posterior edge (to help reduce halos and spokes, squared at the edge to help retard posterior capsular opacification) and the additive Hydroxyethylmethacrylate (HEMA) to slightly increase water content (helping to improve optical clarity and resulting in a glistening-free material).9,*
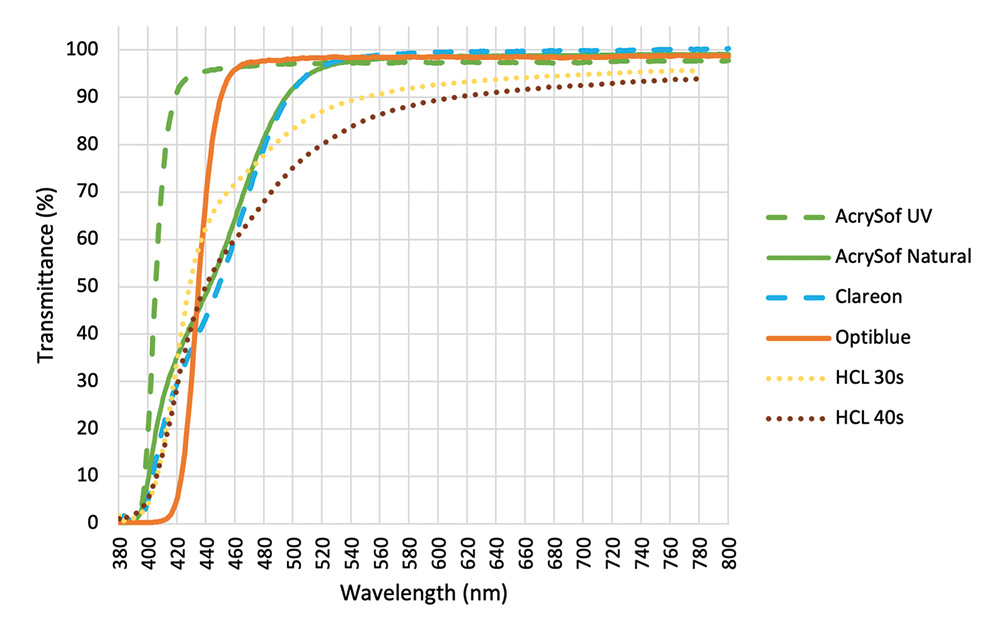
Figure 1. Transmission curves for various BLF IOLs currently[CD2] on the market. The transmittance[IA3] of the Human Crystalline Lens (HCL) at the age of 30s and 40s have been included as reference.8,9
Many of the benefits of the AcrySof Natural IOL are easily reducible to its filtering properties (as shown in the many empirical studies reviewed in the next section). These benefits are also relevant for the Clareon IOL since it utilizes the exact same transmittance profile. The improvements in the design and optical materials used in the Clareon IOL predict that the Clareon IOL will be as good or better than the AcrySof Natural IOL in visual functions. This inference is consistent with optical bench data comparing the modulation transfer functions of the two lenses (shown in Figure 2).10
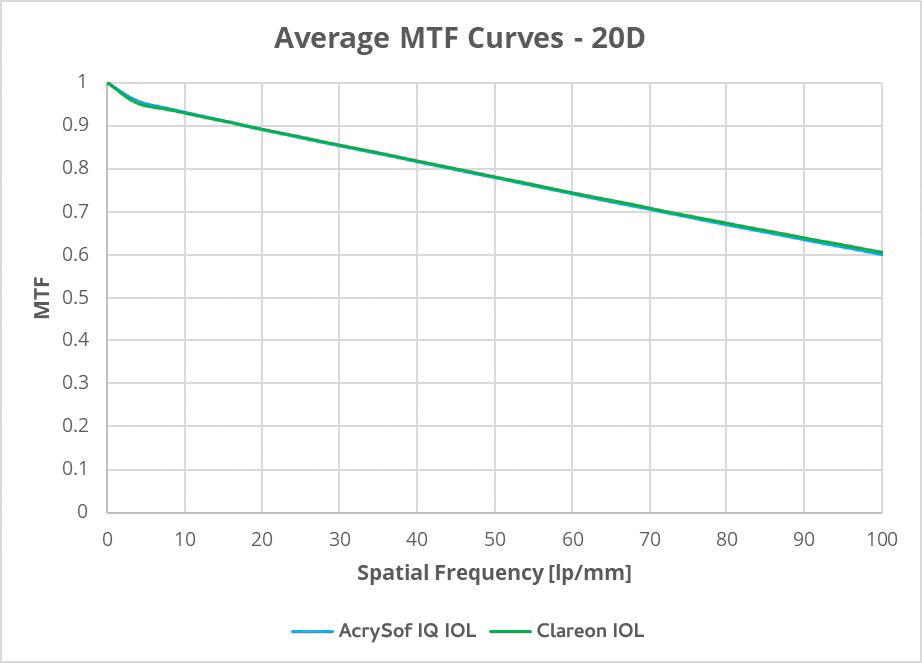
Figure 2. Average MTF Curves for 20.0 D Clareon Monofocal IOL Model SY60WF vs. AcrySof IQ IOL Model SN60WF for 3 mm pupil size.
The effects of IOL type on visual performance
Glare disability & discomfort and photostress recovery
Glare generally refers to the loss of visual performance that accompanies exposure to light that is in excess of an individual’s adaptive state, as originally described by Holladay and Stiles.11,12 Glare is generally separated into two broad categories, glare discomfort (GDC) and glare disability (GD). GDC refers to the slight pain or discomfort that results from bright light, although it might not imply visual loss. Factors that are known to influence GDC are often linked to the potential damage of the inducing light (e.g., GDC is exaggerated at shorter wavelengths).13 BLFs have been shown to reduce GDC.14,15 In contrast, GD focuses specifically on the loss of visual function arising mostly from intraocular scattered light. Glare is a leading cause of automotive accidents and one of the primary reasons that older individuals stop driving at night.16
Sudden exposure to a bright, bleaching light also causes isomerization of a large fraction of photopigment causing temporary loss of vision. This temporary blindness is a common cause of accidents, especially with older drivers.17 Because photopigment must regenerate in order to recover visual function, photostress recovery is a common physiological assessment that changes with advanced age and metabolic diseases like diabetic retinopathy or macular degeneration.18 Empirical data has consistently found that AcrySof Natural IOL increases photostress recovery speeds by about 20-30% when compared to a non-BLF IOL.19-21
There is evidence that BLF IOLs, such as AcrySof IQ Natural, help to reduce glare and its impact. Hammond et al19 found that subjects with implanted AcrySof Natural IOL with BLF had shorter photostress recovery times and significantly reduced GD (P<0.02) compared with AcrySof UV only IOLs. In a contralateral eye study20 the AcrySof Natural IOL had significantly faster photostress recovery (P<0.04) and reduced GD (P<0.02) compared to the AcrySof UV IOL.
Visual dysphotopsia
Halos are primarily the result of forward light scatter and diffusion arising primarily from the crystalline lens. Starbursts22 stem largely from diffraction and aberrations that arise from small particle scattering along the entire optic axis. With broadband light, the effect is needle-like spokes radiating from the image of the source. Hammond et al23 using both a case-control and a contralateral study design showed that AcrySof Natural IOLs with BLF were associated with a significant reduction in halos and spoke size (decreased symptoms of positive dysphotopsia). This effect, like with other aspects of glare, is likely due to strategic blue-light filtering.
Although blue-light filtering can help reduce visual symptoms (halos and spokes), it does not reduce the cause. The Clareon lens introduced a novel optical edge design (edge curvature and a lack of peripheral non-imaging elements) aimed at reducing the origin of dysphotopsias.24
Chromatic contrast
AcrySof Natural IOLs with BLF have been shown empirically to improve chromatic contrast.20 This finding is consistent with other BLF filters such as natural filters like macular pigment.25 Such an effect should not be confused with the ability to see or discriminate colors. Color perception is very clearly not influenced by BLF IOLs.26
Summary
Most individuals are motivated to get an implant because of visual symptoms (e.g., glare, dysphotopsia, blinding lights at night while driving). One major goal of any implant is simply palliative and should focus on reducing “disease.” One strategy for doing that is to match the characteristics selected by the natural evolution of the mammalian eye, BLF filtering. A significant body of evidence (both direct and indirect) has shown that the AcrySof IQ Natural IOL improves visual function in a variety of conditions that directly reflect the symptom profile of older and pre- and post- cataractous patients. The Clareon IOL utilizes the same filtering profile and is expected to have similar benefits. Many of the design features of the Clareon may reduce the origin of these common issues and further increase its benefits.
© 2023 Alcon Inc. 12/23 IMG-ACI-2300005
1. Youssef PN, Sheibani N, Albert DM. Retinal light toxicity. Eye (Lond).2011;25(1):1-14.
2. Hunter JJ, Morgan JIW, Merigan WH, Sliney DH, Sparrow JR, Williams DR. The susceptibility of the retina to photochemical damage from visible light. Prog Retin Eye Res. 2012;31(1):28-42.
3. Hammond BR, Johnson BA, George ER. Oxidative photodegradation of ocular tissues: beneficial effects of filtering and exogenous antioxidants. Exp Eye Res. 2014;129:135-150.
4. Ouyang Q, Yang J, Hong Z, Wu Y, Xie Y, Wang G. Mechanisms of blue light-induced eye hazard and protective measures: a review. Biomed Pharmacother. 2020:130:110577.
5. Algvere PV, Marshall J, Seregard S. Age-related maculopathy and the impact of blue light hazard. Acta Ophthalmol Scand. 2006;84(1):4-15.
6. Grossweiner LI. Photochemistry of proteins: a review. Curr Eye Res. 1984;3(1):137-144.
7. Zigman S, Datiles M, Torczynski E. Sunlight and human cataracts. Invest Ophthalmol Vis Sci. 1979;18(5):462-467.
8. Artigas JM, Felipe A, Navea A, Fandiño A, Artigas C. Spectral transmission of the human crystalline lens in adult and elderly persons: color and total transmission of visible light. Invest Ophthalmol Vis Sci. 2012;53(7):4076-4084.
9. Lehmann R, Maxwell A, Lubeck DM, Fong R, Walters TR, Fakadej A. Effectiveness and safety of the Clareon monofocal intraocular lens: outcomes from a 12-month single-arm clinical study in a large sample. Clin Ophthalmol. 2021;15:1647-1657.
10. Alcon Data on File. A01970-231151. Oct 2023.
11. Holladay LL. The fundamentals of glare and visibility. J Opt Soc Am & Rev Sci Instrum. 1926;12(4):271-319.
12. Stiles WS. The nature and effects of glare. Illum Eng. 1929;22:304–312.
13. Stringham JM, Fuld K, Wenzel AJ. Action spectrum for photophobia. J Opt Soc Am A Opt Image Sci Vis. 2003;20(10):1852-1858.
14. Wenzel AJ, Fuld K, Stringham JM, Curran-Celentano J. Macular pigment optical density and photophobia light threshold. Vision Res. 2006;46(28):4615-4622.
15. Renzi-Hammond LM, Hammond Jr BR. Blue-light filtering intraocular implants and darker irises reduce the behavioral effects of higher-order ocular aberrations. Curr Eye Res. 2022;47(5):753-758.
16. Janoff M. Toward development of a visibility model for roadway lighting design. J. Illum. Eng. Soc. 1993;22:122–130.
17. Mainster MA, Timberlake GT. Why HID headlights bother older drivers. Br J Ophthalmol. 2003;87:113-117.
18. Wu G, Weiter JJ, Santos S, Ginsburg L, Villalobos R. The macular photostress test in diabetic retinopathy and age-related macular degeneration. Arch Ophthalmol. 1990;108(11):1556-1558.
19. Hammond BR, Bernstein B, Dong J. The effect of the AcrySof natural lens on glare disability and photostress. Am J Ophthalmol. 2009;148(2):272-276.
20. Hammond Jr BR, Renzi LM, Sachak S, Brint SF. Contralateral comparison of blue-filtering and non-blue-filtering intraocular lenses: glare disability, heterochromatic contrast, and photostress recovery. Clin Ophthalmol. 2010;4:1465-1473.
21. Hammond BR. Attenuating photostress and glare disability in pseudophakic patients through the addition of a short-wave absorbing filter. J Ophthalmol. 2015;2015:607635.
22. Xu R, Thibos LN, Lopez-Gil N, Kollbaum P, Bradley A. Psychophysical study of the optical origin of starbursts. J Opt Soc Am A Opt Image Sci Vis. 2019;36(4):B97-B102.
23. Hammond BR, Gardner CR, Renzi-Hammond L. The effects of blue-light filtering intraocular implants on glare geometry. Curr Eye Res. 2023;48(7):639-644.
24. Werner L, Thatthamla I, Ong M, et al. Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. J Cataract Refract Surg. 2019;45(10):1490-1497.
25. Renzi LM, Hammond BR. The effect of macular pigment on heterochromatic luminance contrast. Exp Eye Res. 2010:91(6):896-900.
26. Hammond BR, Wooten BR, Saint SE, Renzi-Hammond L. The effects of a blue-light filtering versus clear intraocular implant on color appearance. Transl Vis Sci Technol. 2021;10(12):25.
Important Product Information - AcrySof and Clareon® Family of IOLs
Refer to the Directions for Use labeling for a complete list of indications, warnings and precautions.
