
Performing cataract surgery in a patient who has glaucoma or who is taking IOP-lowering medication is a very common clinical scenario. In the United Kingdom, we've adopted combined procedures at a fairly significant rate, and we now have enough data to answer the question of whether patients gain benefit from the simultaneous placement of an iStent inject® W (Glaukos Corp.) or other trabecular bypass stent versus doing cataract surgery alone. Due to these volumes, I think we can now say there is a new gold standard of glaucoma management in which we consider surgical IOP control, if medically appropriate, in eyes requiring cataract surgery.
Combined Cataract and MIGS Procedures: No Longer a Question of Benefit
From my own experience and patients' outcomes, when I seek the safest and most effective options for lowering IOP that won’t negate other interventions the patient might need in the future, the iStent inject® W (Glaukos Corp.) fits into that category of treatment nicely. For example, the pivotal study for the iStent inject®, published in 2019, was a prospective, multicenter, randomized, controlled trial of 505 total patients who were randomized 3:1 to receive either phacoemulsification and the iStent inject® (n=387), or phacoemulsification alone (n=118). Patient follow-up was performed over 2 years, with annual washouts. The study met its effectiveness endpoints: (primary) a reduction of ≥ 20% in unmedicated diurnal IOP and (secondary) a mean reduction in unmedicated diurnal IOP (Figure 1).1 Furthermore, the treatment group’s safety profile was favorable and similar to that of the control group throughout the 2-year follow-up.
In contrast, the effect of phacoemulsification alone on open-angle glaucoma is likely attenuated from 2 years on.2 Meaning, although cataract surgery alone may lower IOP initially, the effect is not necessarily permanent.

Figure 1. The pivotal study for the iStent inject® met its primary and secondary endpoints.
In a meta-analysis of 13 studies (778 eyes) of iStent implantation alone out to 5 years, Healey et al found that the iStent provided well-sustained reduction in IOP, as well as reduced medication usage.3 Reducing medication usage is important, not only because of the issues of toxicity and compliance, but across the UK, we've seen real challenges to the supply chain of some of the most commonly used drops. Healey et al found a 60% reduction in medication dependence, which is the average of what we see across iStent trials. In turn, removing this insult to the ocular surface would likely push scores on the Ocular Surface Disease Index much more towards the range of normal and mild.
For those patients who've been on the traditional pathway of glaucoma diagnosis, (topical medication then surgery), we want to maximize the chance of surgical success should they need filtration later on. Again, in the clinical trials with the longest-term follow-up of patients receiving an iStent implant, the device reduced patients’ medication burden, more so than other factors.4-7
Quality-of-Life Measurements With iStent
Some of the key takeaways from this year’s EGS plenary session were new goals for designing future clinical trials in glaucoma. It was agreed that outcomes should target at least a 20% reduction in medications for patients, if not complete elimination.
Because it was the first MIGS device brought to market, the iStent inject® is the only drainage device that has pivotal trial data showing significant durable improvements in vision-related quality-of-life measurements.8 The device also has subjective patient data on metrics like general vision, ocular pain, and driving. But what's most exciting, although relatively new, are functional measures.
A meta-analysis conducted by Gillmann et al produced evidence that the iStent slows the rate of functional vision loss (Figure 2).9 That's interesting; we've not really seen this outcome until very recently, and it warrants further research and debate. Still, it helps us give patients more information about what might happen if their IOP control is suboptimal, and how we can influence it.

Figure 2. Researchers compared the observed visual field mean deviation progression following implantation of iStent technologies (pink line) with the rates of progression reported in the literature for ocular hypertension (blue lines) and glaucoma (green lines). (Data adapted from Gillmann K, et al. BMJ Open Ophthalmology. 2024.9)
My colleagues and I at Imperial College reviewed our 5-year results in an observational, retrospective, single-center, longitudinal cohort study of 47 patients who received the first-generation iStent at the time of cataract surgery. Our control group was 44 patients who had undergone cataract surgery alone. We found that IOP was reduced in both groups immediately after surgery, but the cataract-alone patients needed increasing medications over 5 years of follow-up to maintain their target IOPs (Figure 3). Those who received the first-generation iStent had a lower medication burden at 5 years (Figure 3).

Figure 3. The author and her colleagues reviewed their 5-year results on IOP and medication usage in patients who underwent cataract surgery with the first-generation iStent (n=47) versus cataract surgery alone (n=44). Patients who had received the iStent had a greater reduction in IOP and required fewer medications at 5 years.
Perhaps more exciting were the data from our visual field analysis: those who had the iStent experienced a stabilization of their visual field—we didn't see further significant loss or further reduction in the mean deviation. In contrast, the visual fields of those who underwent cataract surgery alone deteriorated (Figure 4). These data reflect previous reports that even patients who receive regular follow-up care can lose their visual field function over time. And again, even though our patients tell us that they take the drops every day, we know from a multitude of evidence that they don’t. So, removing that patient-dependent factor should translate into longer-term visual field stabilization. In our study, 26% of patients were medication-free at 5 years.
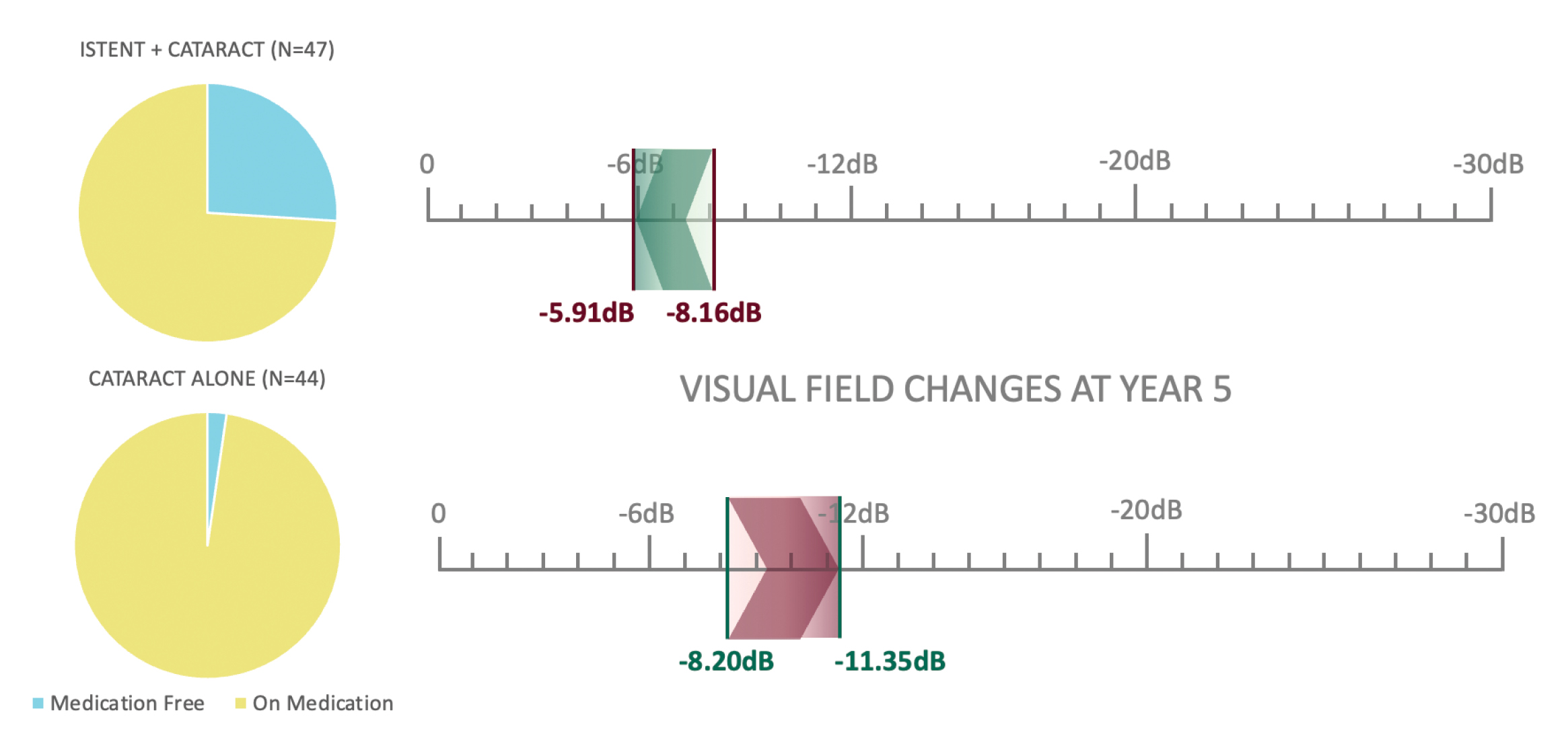
Figure 4. An observational, longitudinal, 5-year outcome for the change in visual field mean deviation before and after cataract surgery combined with the first-generation iStent (n=47) versus cataract surgery alone (n=44). The two groups were matched for age, visual field mean deviation, and glaucoma diagnosis. (Glaucoma Unit, Imperial College Healthcare, NHS Trust, unpublished data.)
CONCLUSION
In summary, I think the safety and efficacy of the iStent inject® W has been proven in both randomized control trials and in the real-world setting. I believe this device offers not only significant benefits for our patients, but for us surgeons, as well as for the healthcare system at large and the financial model within which we have to operate. The iStent inject® W procedure is incredibly elegant and safe, and I think it should be among our first considerations for cataract surgery patients with high IOP, controlled or not. It feels like a missed opportunity if we don't offer a secondary procedure that does not have an impact on the cataract surgical procedure but can potentially change the patient’s quality of life and/or their treatment outcome.
To hear more from Dr. Crawley, visit https://eyetube.net/spotlight/glaukos-international/glaukos-egs-symposium-2024-video-3
1. Samuelson TW, Sarkisian Jr SR, Lubeck DM, et al. Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology. 2019;126(6):811-821.
2. Armstrong JJ, Wasiuta T, Kiatos E, et al. The effects of phacoemulsification on intraocular pressure and topical medication use in patients with glaucoma: a systematic review and meta-analysis of 3-year data. J Glaucoma. 2017;26:511–522.
3. Healey PR, Clement CI, Kerr NM, et al. Standalone iStent trabecular micro-bypass glaucoma surgery: a systematic review and meta-analysis. J Glaucoma. 2021;30(7):606-620.
4. Hengerer FH, Auffarth GU, Conrad-Hengerer I. 7-year efficacy and safety of istent inject trabecular micro-bypass in combined and standalone usage. Adv Ther. 2024;41(4):1481-1495.
5. Salimi A, Watt H, Harasymowycz P. Long-term outcomes of two first-generation trabecular micro-bypass stents (iStent) with phacoemulsification in primary open-angle glaucoma: eight-year results. Eye Vis (Lond). 2021;8(1):43.
6. Neuhann TH, Neuhann RT, Hornbeak DM. Ten-year effectiveness and safety of trabecular micro-bypass stent implantation with cataract surgery in patients with glaucoma or ocular hypertension. Ophthalmol Ther. Published online ahead of print June 21, 2024.
7. Ferguson TJ, et al. Trabecular micro-bypass stent implantation with cataract surgery in open-angle glaucoma: 9 year results. Presented at: the ASCRS Symposium on Cataract, IOL and Refractive Surgery; May 5-8, 2023; San Diego, CA.
8. Samuelson TW, Singh IP, Williamson BK, et al. Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ-25 and OSDI from the iStent inject® pivotal trial. Am J Ophthalmol. 2021;229:220-229.
9. Gillman K, Hornbeak DM. Rates of visual field change and functional progression in glaucoma following trabecular microbypass implantation of iStent technologies: a meta-analysis. BMJ Open Ophthalmol. 2024;9(1):e001575. Published online ahead of print Feb 15, 2024.

INDICATIONS FOR USE: The iStent inject® is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject® can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject® System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS: • For prescription use only. • This device has not been studied in patients with uveitic glaucoma. • Do not use the devices if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent inject® is MR-Conditional; see MRI Information below. • Physician training is required prior to use of the iStent inject® System. • Do not re-use the stent(s) or inserter, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events as shown below under “Potential Complications.” • There are no known compatibility issues with the iStent inject® and other intraoperative devices (e.g., viscoelastics) or glaucoma medications. • Unused product & packaging may be disposed of in accordance with facility procedures. Implanted medical devices and contaminated products must be disposed of as medical waste. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body • The surgeon should monitor the patient postoperatively for proper maintenance of intraocular pressure. If intraocular pressure is not adequately maintained after surgery, the surgeon should consider an appropriate treatment regimen to reduce intraocular pressure.
INDICATION FOR USE: The iStent inject® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations. • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS: • For prescription use only. • This device has not been studied in patients with uveitic glaucoma. • Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent inject® W is MR-Conditional; see MRI Information below. • Physician training is required prior to use of the iStent inject® W System. • Do not re-use the stent(s) or injector, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events as shown below under “Potential Complications.” • There are no known compatibility issues with the iStent inject® W and other intraoperative devices. (e.g., viscoelastics) or glaucoma medications. • Unused product & packaging may be disposed of in accordance with facility procedures. Implanted medical devices and contaminated products must be disposed of as medical waste. • The surgeon should monitor the patient postoperatively for proper maintenance of intraocular pressure. If intraocular pressure is not adequately maintained after surgery, the surgeon should consider an appropriate treatment regimen to reduce intraocular pressure. • Patients should be informed that placement of the stents, without concomitant cataract surgery in phakic patients, can enhance the formation or progression of cataract. ADVERSE EVENTS: Please refer to Directions For Use for additional adverse event information. CAUTION: Please reference the Directions For Use labelling for a complete list of contraindications, warnings and adverse events.
© 2024 Glaukos Corporation. Glaukos, iStent inject® and iStent inject® W are registered trademarks of Glaukos Corporation. PM-EU-0310
