
We’ve now entered a stage in glaucoma management where we must ask: when do we cut, when do we dilate, when do we stent, and when do we combine? As Dr. Gillmann described earlier, each approach has its strengths and weaknesses. We’ve moved from a time of single-device use to broader placement strategies with multiple implants, as seen with the iStent infinite® (Glaukos Corporation).
When we think about outflow, it’s fundamentally about access to the collector channels. Across preclinical, basic science, and clinical data, the iStent infinite® demonstrates greater efficacy, particularly when used in combined phacoemulsification (phaco) procedures, which have driven much of the innovation in North America. Globally, however, combined MIGS remains underutilized. I hope that this message resonates: combining MIGS with cataract surgery early can profoundly improve patient outcomes.
Safety and Evolution of Microstents
When MIGS first emerged, what truly distinguished it from traditional glaucoma surgery was its safety, especially when combined with phaco. While efficacy can be debated, trabecular microstents remain the safest approach, minimizing tissue trauma and hyphema.
We’ve seen the evolution of iStent®, with evidence continuing to build. The concept of multiple stents originated early, with data showing that broader canal access provides better results. The single stent established safety; as we moved from two to three stents, we maintained that safety while improving efficacy, efficiency, and predictability of delivery.
Surgical Technique
I will describe my technique with the iStent infinite® in a standalone procedure in a pseudophakic eye with capsular fibrosis. Each stent accesses roughly two clock hours of outflow, so it’s ideal to place them two to three clock hours apart for maximal coverage. That requires adjusting your microscope angle and head position to achieve the correct entry angle.
I still prefer to implant left to right, although either direction works. The key is to aim for the top of the trabecular meshwork (TM). Because we enter with a negative angulation, we must ensure the stent isn’t implanted too deep—one of the most common mistakes.
It’s also about pressure control: if you press too lightly, you under-implant; too firmly, you risk over-implantation. The iStent infinite®, with its large flange, helps prevent that. My rule is to press with enough force to create a “U” pattern, not a “V”—a gentle curve ensures optimal placement (Figure 5). Then I release smoothly, pulling back in line to avoid dislodging the stent.
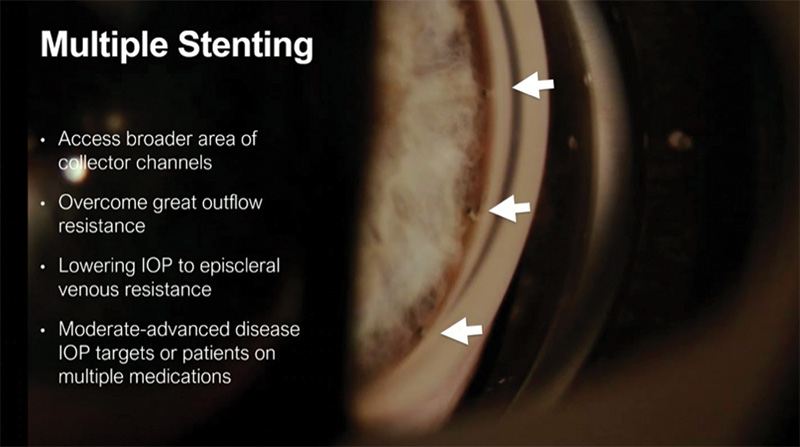
Figure 5. Proper angulation and spacing for multi-stent placement in Schlemm’s canal.
Next, I swing the scope several clock hours to place the next stent. Again, I approach the top of the TM, apply gentle depression, and check that the trocar isn’t biased or twisted. Stability of the anterior chamber results from retaining viscoelastic—the retractable sleeve seals the incision, preventing leakage. I rotate my hand and scope to reach wider, placing the stents farther apart than I do with the iStent inject® W to access broader canal segments.
For those just starting to learn this technique, it’s fine to place the stents closer together until confidence builds. As you gain experience, wider placement improves outflow. Some surgeons even use a sub-nasal incision to place one stent temporally, expanding access.
Real-World Data
My team and I recently analyzed real-world data from my practice on combined phaco with iStent infinite®.15 This was not a controlled study, but it provides meaningful insight into outcomes across diverse glaucoma types, including advanced cases and some off-label diagnoses.
We defined success as the proportion of patients achieving medication reduction without increased IOP, or ≥20% IOP reduction with equal or fewer medications. Any eye requiring further surgery was excluded from the success rate.
Baseline mean IOP of 15.9 mm Hg decreased to 13.4 mm Hg postoperatively. Medications dropped from 1.7 to 0.8 on average (Figure 6). We observed an 87% primary success rate at 1 year, with no patients experiencing IOP increases. A few had early postoperative IOP spikes—likely steroid-related—but these resolved with management.
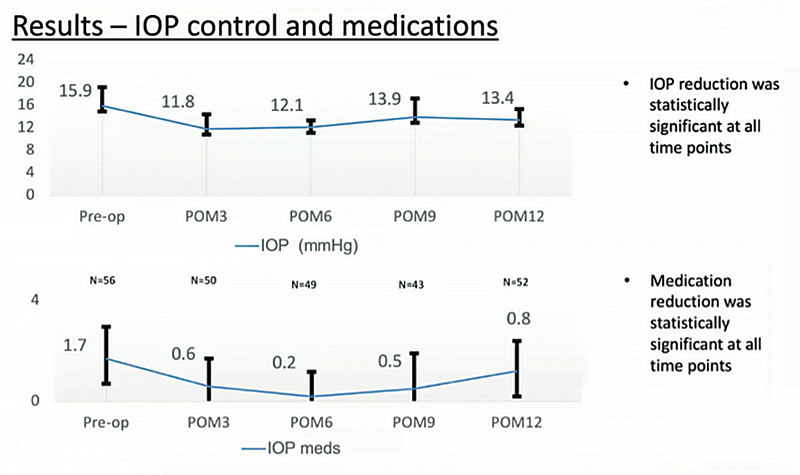
Figure 6. One-year medication and IOP outcomes from an uncontrolled, single-site, retrospective analysis of patients treated with the iStent infinite and phacoemulsification.15
These findings confirm what we’ve seen across studies: the iStent infinite® maintains the hallmark safety of earlier iStent technologies while enhancing IOP and medication reduction.
The Case for Earlier Intervention
I want to emphasize that earlier intervention works better. Both MIGS and SLT demonstrate superior outcomes when performed early, before irreversible outflow or optic nerve damage occurs. So, think about offering these procedures sooner in the patient’s journey. Not every patient will choose surgery, but every glaucoma patient should be offered the option—especially when combined with phaco.
Although standalone MIGS remains a small portion of the market, especially outside North America, its role is growing. The iStent infinite® is supported by high-quality, prospective, randomized data, unlike much of the lower-quality MIGS literature. We must prioritize evidence-based decision-making while balancing effort, risk, cost, and efficacy, and continue building the evidence base for interventional glaucoma.
1. Mehrdad M, Moura Filho ER, Hodge DO, et al. Long-term trends in glaucoma-related blindness in Olmsted County, Minnesota. Ophthalmology. 2014;121(1):134-141.
2. Peters D, Bengtsson B, Heijl A. Lifetime risk of blindness in open-angle glaucoma. Am J Ophthalmol. 2013;156(4):724-730.
3. Nordstrom BL, Friedman DS, Mozaffari E, et al. Persistence and adherence with topical glaucoma therapy. Am J Ophthalmol. 2005;140(4):598-606.
4. Analysis of market, claims, and compliance data. Data on file. Glaukos Corporation.
5. Sarkisian SR Jr, Ang RE, Lee AM, et al. Phase 3 randomized clinical trial of the safety and efficacy of travoprost intraocular implant in patients with open-angle glaucoma or ocular hypertension. Ophthalmology. 2024;131(9):1021-1032.
6. Sarkisian SR, Ang RE, Lee AM, et al. Travoprost intracameral implant for open-angle glaucoma or ocular hypertension: 12-month results of a randomized, double-masked trial. Ophthalmol Ther. 2024;13(4):995-1014.
7. Williams AM, Wasser LM, Cassidy J, Lin HS. Loss to follow up among glaucoma patients: An IRIS® Registry (Intelligent Research in Sight) retrospective cohort analysis. Semin Ophthalmol. 2025;40(3):188-195.
8. Williams AM, Liang HW, Lin HHS. Loss to follow-up and risk of incident blindness among patients with glaucoma in the IRIS® Registry (Intelligent Research in Sight). Ophthalmol Glaucoma. 2025:S2589-4196(25)00104-8. Published online May 2, 2025.
9. Funke C, Ristvedt D, Yadgarov A, Micheletti JM, for the Interventional Glaucoma Working Group. Interventional glaucoma consensus treatment protocol. Exp Rev Ophthalmol. 2025;20(4):1-9.
10. Gillmann K, Lallouette A, Baudouin C, et al. A systematic and narrative review of safety and complications in minimally invasive glaucoma surgery (MIGS) between 2014–2024. Clin Ophthalmol. Submitted for publication.
11. Ahmed IIK, Sheybani A, DeFrancesco T, et al. Corneal endothelial safety profile in minimally invasive glaucoma surgery. J Cataract Refract Surg. 2023;50(4):369–377.
12. Samuelson TW, Chang DF, Marquis R, et al. A Schlemm canal microstent for intraocular pressure reduction in primary open-angle glaucoma and cataract. Ophthalmology. 2019;126(1):29-37.
13. Sarkisian SR Jr, Grover DS, Gallardo MJ, et al. Effectiveness and safety of iStent infinite trabecular micro-bypass for uncontrolled glaucoma. J Glaucoma. 2023;32(1):9-18.
14. Ahmed IK, Berdahl JP, Yadgarov A, et al. Six-Month Outcomes from a Prospective, Randomized Study of iStent infinite Versus Hydrus in Open-Angle Glaucoma: The INTEGRITY Study. Ophthalmol Ther. 2025;14(5):1005-1024.
15. Siempis T, Varma D, Schlenker M, Ahmed I. Real world clinical outcomes of combined phacoemulsification and iStent® Infinite TM bypass implantation in a heterogeneous population. Presented at: The winter meeting of the ESCRS. February 2025; Copenhagen, Denmark.
INDICATION FOR USE: The iStent inject® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations. • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS: • For prescription use only. • This device has not been studied in patients with uveitic glaucoma. • Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent inject® W is MR-Conditional; see MRI Information below. • Physician training is required prior to use of the iStent inject® W System. • Do not re-use the stent(s) or injector, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events as shown below under “Potential Complications.” • There are no known compatibility issues with the iStent inject® W and other intraoperative devices. (e.g., viscoelastics) or glaucoma medications. • Unused product & packaging may be disposed of in accordance with facility procedures. Implanted medical devices and contaminated products must be disposed of as medical waste. • The surgeon should monitor the patient postoperatively for proper maintenance of intraocular pressure. If intraocular pressure is not adequately maintained after surgery, the surgeon should consider an appropriate treatment regimen to reduce intraocular pressure. • Patients should be informed that placement of the stents, without concomitant cataract surgery in phakic patients, can enhance the formation or progression of cataract. ADVERSE EVENTS: Please refer to Directions For Use for additional adverse event information. CAUTION: Please reference the Directions For Use labelling for a complete list of contraindications, warnings and adverse events.
INDICATION FOR USE. The iStent infinite System is intended to reduce intraocular pressure safely and effectively in adult patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The device is safe and effective when implanted in combination with or without cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and/or conventional glaucoma surgery. CONTRAINDICATIONS: The iStent infinite System is contraindicated under the following circumstances or conditions: •In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations.• In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure WARNINGS/PRECAUTIONS: • For prescription use only. • Intended users are trained ophthalmologists only. • This device has not been studied in patients with uveitic glaucoma. • Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e., the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent infinite is MR-Conditional • Physician training is required prior to use of the iStent infinite System. • Do not re-use the stent(s) or injector, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events • There are no known compatibility issues with the iStent infinite and other intraoperative devices (e.g., viscoelastics) or glaucoma medications. • Unused product & packaging may be disposed of in accordance with facility procedures. Implanted medical devices and contaminated products must be disposed of as medical waste. • The surgeon should monitor the patient postoperatively for proper maintenance of intraocular pressure. If intraocular pressure is not adequately maintained after surgery, the surgeon should consider an appropriate treatment regimen to reduce intraocular pressure. • Patients should be informed that placement of the stents, without concomitant cataract surgery in phakic patients can enhance the formation or progression of cataract. ADVERSE EVENTS: The most common postoperative adverse events reported in the iStent infinite pivotal trial included IOP increase ≥ 10 mmHg vs. baseline IOP (8.2%), loss o f BSCVA ≥ 2 lines (11.5%), ocular surface disease (11.5%), perioperative inflammation (6.6%) and visual field loss ≥ 2.5 dB (6.6%). CAUTION: Please see DFU for a complete list of contraindications, warnings, precautions, and adverse events.
For additional safety information on iStent products, see here: www.glaukos.com
Glaukos®, iStent®, iStent inject®, iStent inject® W and and iStent infinite® are registered trademarks of Glaukos Corporation. All rights reserved. ©2026. Third-party trademarks are the property of their respective owners. PM-EU-0391
