
A roundtable discussion was given by dry eye experts during the European Dry Eye Congress (EUDEC) in June 2022 in collaboration with Quantel Medical. The roundtable was broadcast online on the European Dry Eye Disease Society (EUDES) website (https://www.dryeye-society.com/dry-eye-live-talks).
INTRODUCTION
Prof. Dr. Elisabeth M. Messmer: Intense pulsed light (IPL) is a new and emerging technique for the treatment of dry eye disease (DED).
PHYSICAL BASICS OF INTENSE PULSED LIGHT (IPL)
Prof. Dr. Messmer: Dr. Doan, what do we know about the physical basics of IPL?
Serge Doan, MD: The principle of IPL is to create a thermal effect with a very intense flash of light. The treatment was initially intended for dermatological use, mainly for rosacea to flush the telangiectasia, but more recently it has been adapted for use in dry eye. For ophthalmic use, IPL systems deliver a flash of light to the skin adjacent to the eyes at a lower intensity than dermatological IPL devices use to ensure that the eyelids will not be affected. The treatment is intended for the management of dry eye disease (DED) related to meibomian gland dysfunction (MGD).
The C.STIM® Intense Pulsed Light System (Quantel Medical by Lumibird Medical) uses polychromatic, noncoherent (i.e., different from laser) small pulses of uniform light intensity (Figure 1). During the IPL treatment, trains of 4- to 5-millisecond flashes of white or red light are applied around or directly onto the eyelids.
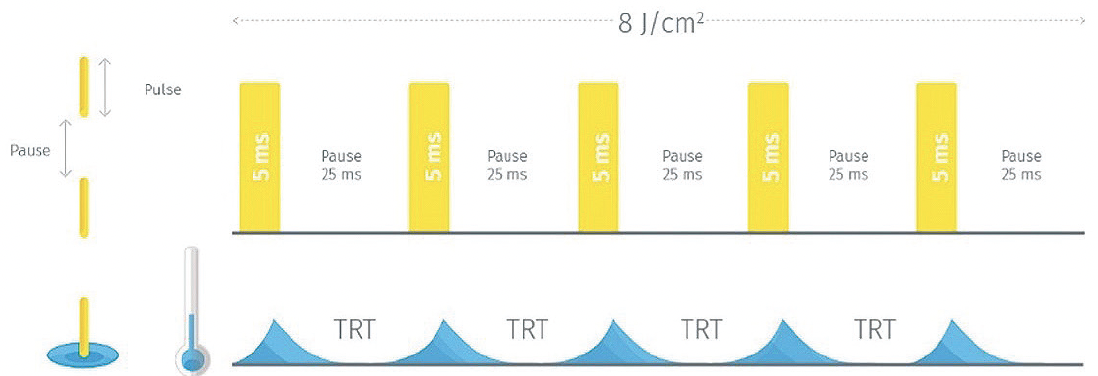
Figure 1. Train pulse.
MECHANISM OF ACTION OF IPL
Prof. Dr. Messmer: What is the mechanism of action of IPL for the management of DED?
Dr. Doan: The exact mechanism is unknown. The energy of the IPL flash is absorbed by tissues, and the temperature increases in the treated area. This could lead to liquefying of the meibum or the absorption of the light in the red blood cell could collapse the telangiectasic vessels of the lid margin and affect parasites such as Demodex1 and other microorganisms that are in that same area. Interestingly, anti-inflammatory effects with a decrease of many inflammatory markers in the tears have been shown.2-7 It is not clear whether some photo biomodulation occurs within the tissue because this effect is mainly obtained with laser.8
Patients with MGD typically respond well to IPL treatment (Figure 2). It might also be advantageous for patients with aqueous tear deficient DED because of the treatment’s anti-inflammatory effects in the tear film (Figure 3).
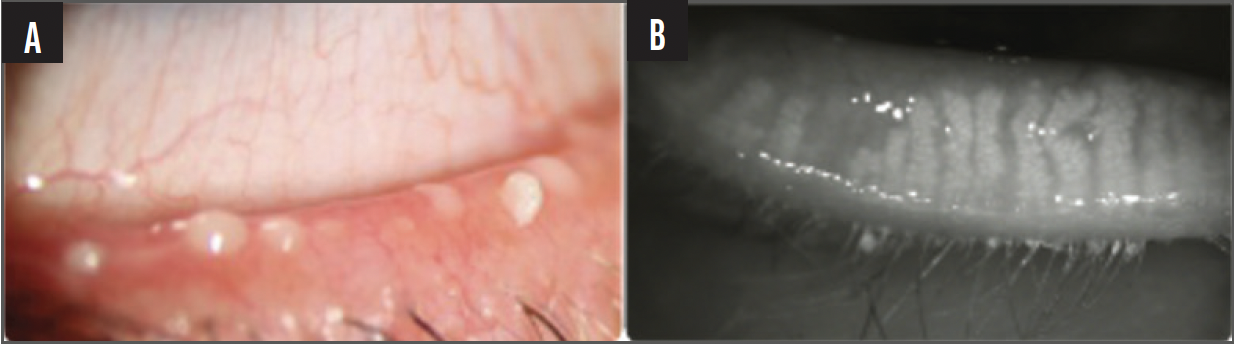
Figure 2. Examples of meibomian gland dysfunction.
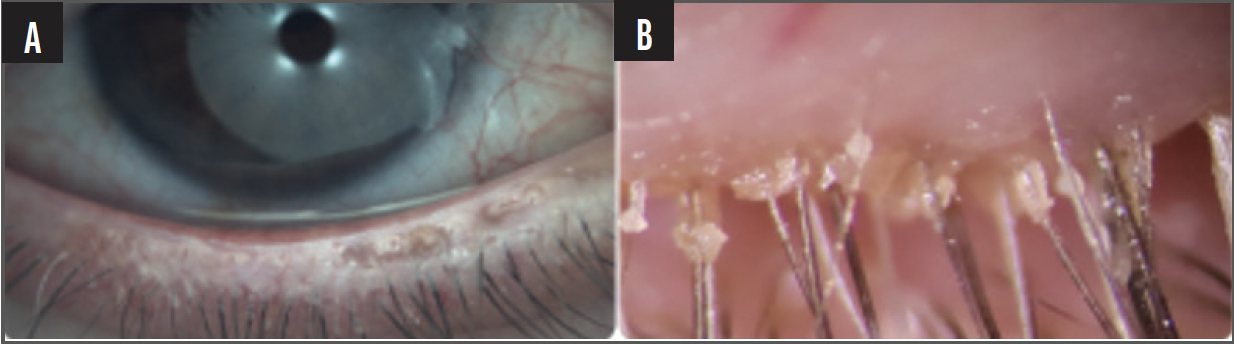
Figure 3. The appearance of inflammation (A) and Demodex (B).
Prof. Dr. Messmer: In my experience, IPL is a very good second-line treatment for patients who have not responded to basic DED therapies, such as artificial tears, lid hygiene, and control of environmental factors.
EXPECTED CLINICAL RESULTS OF IPL
Prof. Dr. Messmer: Studies have shown positive results with IPL for DED management. In the first controlled clinical trial in 2015, Craig et al showed that IPL significantly improved the lipid layer, tear breakup time, and subjective symptoms compared to the partner eye that did not receive IPL treatment.9 Studies conducted on the use of IPL for refractory MGD have had similar positive outcomes.10
IPL AND SJOGREN
Prof. Dr. Messmer: Dr. Lazreg, you use IPL in patients with Sjogren syndrome. What has your experience been?
Sihem Lazreg, MD: I have many patients with Sjogren syndrome and DED who improve significantly after IPL. I agree with you, Professor Messmer, that IPL is not a first-line treatment, but when I supplement a patient's treatment regimen with IPL, they feel significantly better because it decreases ocular surface inflammation. I have experienced the same positive results in patients with ocular allergy.
IPL AND NEUROPATHIC PAIN
Prof. Dr. Messmer: Patients with DED and neuropathic pain can be challenging to treat successfully. Professor Labetoulle, has IPL been a good treatment option for these patients?
Marc Labetoulle, PhD: Neuropathic pain is a significant issue in DED patients. Most of our patients have symptoms of DED that correlate with the signs of the disease, but a huge discrepancy can also occur between symptoms and signs. When the signs are present and the patient does not experience the symptoms of DED, it is crucial to test for neurotrophic keratitis. On the contrary, when the signs are much lower than the patient’s subjective level of symptoms, the clinician should consider a diagnosis of neuropathic pain, which is an inflammatory disease.
Neuropathic pain, triggered by the inflammation of the nociceptors, is just one potential consequence of long-term ocular inflammation. A study published in Biomedicines in 2021 showed that the corneal abnormalities of patients with MGD directly correlated to the level of inflammation in the cornea.11 In eyes with aqueous tear deficient DED, the corneal abnormalities were more pronounced around the nerves with a lot of dendritic cells.
IPL can be such an effective treatment in this population because it reduces the tear’s inflammatory markers, including interleukin-17. We are currently conducting a trial at Bicetre- Hospital (Paris-Saclay University) to determine the effects of IPL treatment on the ocular surface of patients with mild to moderate MGD combined with underlying neuropathic pain. In our preliminary results, we observed an improvement in the signs and symptoms of DED as determined by the Ocular Surface Disease Index (OSDI) questionnaire and the Oxford corneal score. We believe these first results suggest that IPL may be a logical treatment to address neuropathic pain observed in the context of mild to moderate MGD.
Prof. Dr. Messmer: Professor Labetoulle, could IPL have a direct effect on ocular surface innervation?
Prof. Labetoulle: By modifying the inflammatory factors around the nerves, IPL is expected to help reduce the pathogenesis of the neuropathic pain, which is the consequence of auto excitation of the nociceptors by the surrounding inflammatory environment. When these receptors are inflamed for an extended time, the channels are modified and no longer need any stimulus to trigger pain. When inflammation decreases, such as after IPL, it helps to reverse these abnormalities in the nociceptors.
As a proof of concept, in most cases of post-LASIK DED with neuropathic pain, IPL has been described as improving quality of life by decreasing level of pain.12
IPL AND CATARACT SURGERY
Prof. Dr. Messmer: That has been my experience as well. IPL has also been used in patients who present with MGD prior to cataract surgery. In these patients, the first IPL session was typically performed 4 to 6 weeks before cataract surgery, with two treatments after cataract surgery—one at 1 month and one at 2 months postoperatively.
In a 2020 study by Ge et al, 60 patients scheduled for cataract surgery. Those who received one IPL treatment prior to surgery and two treatments after surgery had fewer symptoms of dry eye and reduced corneal staining, as well as better meibomian gland anatomy and secretions, compared to patients who had undergone cataract surgery alone.13
PREFERRED PROTOCOLS FOR IPL TREATMENT
Prof. Dr. Messmer: Who performs IPL in combination with other DED treatments?
Sihem Lazreg, MD: I always combine IPL with other treatments. My first-line treatment is always lid hygiene and manual expression of the meibomian glands with forceps or automatic brushes to clean the lid margins (Figure 4). The latter is very useful in the pediatric population because the lid margin is so difficult to clean.

Figure 4. Manual expression of the meibomian glands.
I prefer to first clean the eyelid border and express the glands, then perform the treatment with IPL. For me, this method is more convincing and with fewer complications. I perform the eyelid hygiene and then apply the IPL 1 to 2 weeks later. I apply the second IPL 2 weeks after, and then I wait a month for the final IPL session.
Prof. Dr. Messmer: Do you feel comfortable combining IPL with oral doxycycline treatment? We know that doxycycline may increase toxicity to light and some physicians consider discontinuing it during IPL treatment.
Dr. Lazreg: I would be comfortable using them in combination in adult patients with rosacea. If they do not have rosacea or if they are pediatric patients, I prefer topical azithromycin.
Prof. Dr. Messmer: How do you perform IPL treatment?
Dr. Lazreg: Three cycles, one each on Day 0, Day 15, and Day 45. Then, after a year, I can do another sequence.
Prof. Dr. Messmer: Dr Doan, how do you perform IPL treatment?
Dr. Doan: I typically prefer three cycles of IPL. The first and second cycles are performed around the eyes (patient should use goggles). If it works, I continue with one or two more cycles, spaced about 2 weeks apart. If it does not work, I continue with one or two more cycles spaced about 1 month apart, but I apply the flashes directly onto the eyelids after having inserted a protective scleral shell. In my experience, treatment usually works for patients for about 4 to 6 months before repeat treatment is required.
Prof. Dr. Messmer: I like the idea of treating the upper eyelid. Normally we mainly give attention to the lower eyelid, but with your technique, you can also target the upper eyelid.
Dr. Doan: I use the scleral shell to protect the eye, and I decrease the energy to avoid problems with the eyebrows. The results when treating directly on the upper eyelid are much more effective.
Dr. Lazreg: Treating the upper eyelid can be somewhat difficult since the eyebrows can hinder the treatment and can cause a decrease in hair of the brows.
Dr. Doan: In that case, it is better to decrease the fluency of the treatment in that area.
Prof. Labetoulle: My IPL protocol is to perform two sessions at 2 weeks apart and a third session 2 to 4 weeks later. We have follow-up for MGD patients who experienced a relapse and for those with neuropathic pain through Day 120. Results seen at 1 month after the first treatment tend to drop off about 30 to 40 days after the last session of IPL, suggesting that the effect of IPL on inflammation and neuropathic pain decreases with time. Our results have also shown that the drop-off in efficacy is steeper in symptoms of neuropathic pain compared to clinical signs of MGD. It would therefore appear that the efficacy of IPL for the management of MGD lasts longer than it does for inflammation associated with neuropathic pain.
Prof. Dr. Messmer: My patients typically present again after about 6 months for retreatment. I think that, for MGD patients, 6 months is a good interval to have a second treatment cycle. Many of my patients in Germany come in the fall to prepare their eyes for the colder season.
Dr. Lazreg: Emphasizing proper eyelid hygiene to patients can help to avoid relapses from occurring before 6 months.
Prof. Dr. Messmer: Recent research has shown that IPL may be a treatment option for hordeola and chalazion. Dr. Lazreg, would you like to comment on that?
Dr. Lazreg: I see many children with recurrent chalazions, and in my experience, IPL is a very useful treatment. It can be used to combat the inflammation of the lid margin and the blocked orifices associated with the chalazion.
Prof. Dr. Messmer: I also started using IPL in the early treatment of hordeola and chalazion. The anti-inflammatory effect of IPL seems to work very well in these diseases.
CONCLUSION
Prof. Dr. Messmer: IPL is a wonderful emerging technique for several indications (Figure 5), the most important two being DED and MGD. In the future, it is extremely possible that IPL also will be an important treatment for neuropathic pain and hordeola/chalazion. I hope that you enjoyed our discussion and learned valuable information that you can take back to your daily clinics.

Figure 5. IPL treatment with IPL C.Stim®
(Quantel Medical by Lumibird Medical).
1. Huo Y, Mo Y, Wu Y, Fang F, Jin X. Therapeutic effect of intense pulsed light with optimal pulse technology on meibomian gland dysfunction with and without ocular Demodex infestation. Ann Transl Med. 2021;9(3):238.
2. Byun J, Choi H, Myung K, Choi Y. Expression of IL-10, TGF-beta(1) and TNF-alpha in cultured keratinocytes (HaCaT Cells) after IPL treatment or ALA-IPL photodynamic treatment. Ann Dermatol. 2009;21(1):12-17.
3. Huang J, Luo X, Lu J, et al. IPL irradiation rejuvenates skin collagen via the bidirectional regulation of MMP-1 and TGF-beta1 mediated by MAPKs in fibroblasts. Lasers Med Sci. 2011;26(3):381-387.
4. Wong WR, Shyu WL, Tsai JW, Hsu KH, Lee HY, Pang JH. Intense pulsed light modulates the expressions of MMP-2, MMP-14 and TIMP-2 in skin dermal fibroblasts cultured within contracted collagen lattices. J Dermatol Sci. 2008;51(1):70-73.
5. R Lui. Am J Ophthalmol. 2017
6. Lee H, Han YE, Park SY, et al. Changes in the expression of matrix metalloproteinase-9 after intense pulsed light therapy combined with meibomian gland expression in moderate and severe meibomian gland dysfunction. Cont Lens Anterior Eye. 2021;44(3):101339.
7. Li Q, Liu J, Liu C, Piao J, Yang W, An N, Zhu J. Effects of intense pulsed light treatment on tear cytokines and clinical outcomes in meibomian gland dysfunction. PLoS One. 2021;16(8):e0256533.
8. H Chung, The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2012;40(2):516-533.
9. Xue AL, Wang MTM, Ormonde SE, Craig JP. Randomised double-masked placebo-controlled trial of the cumulative treatment efficacy profile of intense pulsed light therapy for meibomian gland dysfunction. Ocul Surf. 2020;18(2):286-297.
10. Arita R et al. Therapeutic efficacy of intense pulsed light in patients with refractory meibomian gland dysfunction. Ocul Surf. 2019;17:104-110.
11. Guerrero-Moreno A, Liang H, Moreau N, et al. Corneal nerve abnormalities in painful dry eye disease patients. Biomedicines. 2021;9(10):1424.
12. Pazo EE, Huang H, Fan Q, et al. Intense pulse light for treating post-LASIK refractory dry eye. Photobiomodul Photomed Laser Surg. 2021;39(3):155-163.
13. Ge J, Liu N, Wang X, et al. Evaluation of the efficacy of optimal pulsed technology treatment in patients with cataract and Meibomian gland dysfunction in the perioperative period. BMC Ophthalmology. 2020;20:111.




