



The goal of refractive cataract surgery is to fully correct the patient’s refractive error and optimize vision quality at all distances. The best strategy by which to achieve this goal may be to implant a premium IOL, but not every patient can afford the technology. In France, a copayment is charged for the correction of astigmatism and/or presbyopia with an IOL. It is the ophthalmologist’s duty to offer the best treatment for each patient, whatever their personal or professional situation.
In 2015, a young man presented to our practice with a unilateral cataract. He was unemployed and had only universal mutual insurance. Without private health insurance, he could not afford the out-of-pocket cost of a premium IOL.
Knowing the patient would benefit from a multifocal IOL, I (G.L.) contacted the former president of the PhysIOL laboratory. With the company’s agreement, I was able to offer the patient a multifocal IOL (FineVision Toric POD FT, now Beaver-Visitec International) for free. It was a win-win-win. The patient was extremely satisfied with his postoperative vision, the company helped a young man see better, and I (G.L.) accomplished my mission to provide the best possible solution to the patient’s vision problem (Figure).
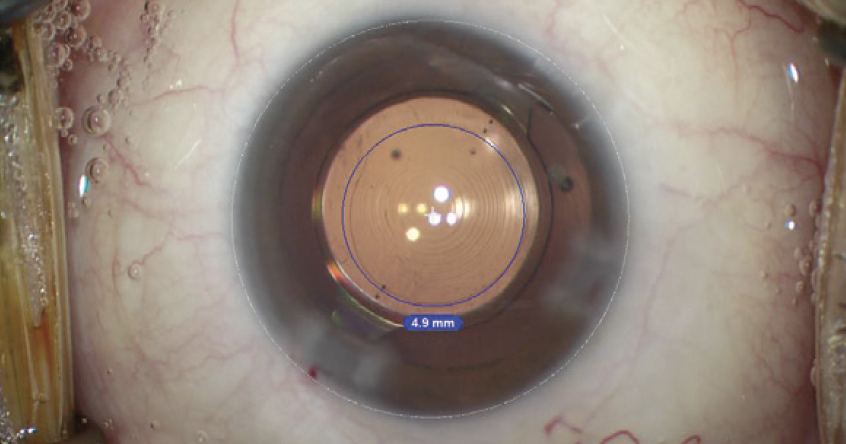
Figure. The FineVision Toric POD FT in situ.
Several years later, the patient developed a cataract in the contralateral eye. By that time, his professional situation had changed. He was working for a painting company and able to afford a premium lens. Surgery went well, and the patient achieved a good quality of vision at both distance and near. PhysIOL, moreover, had a positive return on its investment because the patient chose to receive the same type of IOL implanted in his first eye.
