



As refractive cataract surgeons, our aim is to select the right set of tools and technologies for each patient. This requires a careful analysis of subjective patient factors such as lifestyle, goals, and personality as well as objective measures of the eye’s refractive state and visual potential. Throughout this process, we must consider the regularity or irregularity of the tear film and underlying cornea because this portion of the human optical system accounts for two-thirds of its total refractive power.
CHARACTERIZING IRREGULAR CORNEAS DURING THE CATARACT CONSULTATION
In most eyes free of corneal pathology or scars that have regular astigmatism, higher-order aberrations (HOAs) are minimal. This optimal scenario allows us to consider the full range of IOL technologies for patients seeking premium outcomes. Suboptimal corneal or ocular surface health restricts treatment options.
During a typical cataract surgery consultation, I begin by reviewing the patient’s medical and surgical history for prior corneal refractive surgery (eg, PRK, LASIK, SMILE, or radial keratotomy [RK]) and other ocular surgeries (eg, corneal transplantation or pterygium surgery), ocular trauma, contact lens use or overuse, and ocular diagnoses (eg, Fuchs dystrophy or keratoconus). I inquire about dry eye symptoms with questions such as, “Do you experience intermittent blurring of vision?” I then conduct a thorough slit-lamp examination that focuses on all corneal layers. Each eye is stained with fluorescein dye and viewed under cobalt blue light. This technique facilitates the identification of positive staining abnormalities such as punctate epithelial erosions and negative staining abnormalities such as epithelial basement membrane dystrophy (Figure 1), Salzmann nodular degeneration, and previous cuts and scars.
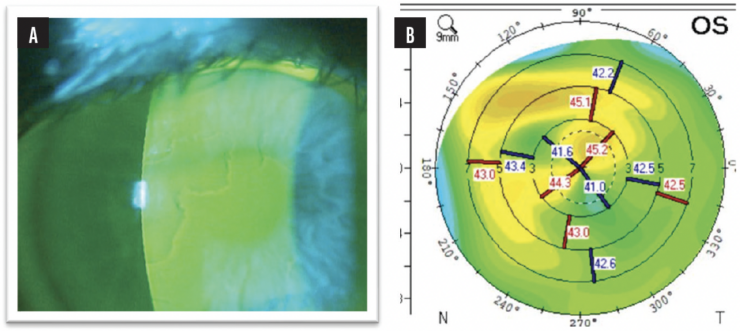
Figure 1. A slit-lamp examination (A) and topography (B) reveal areas of mild irregular astigmatism from epithelial basement membrane dystrophy. Dr. De Rojas would first perform a superficial keratectomy. After healing is complete and the refraction stabilizes, he would consider implanting a premium IOL.
Topography and, if possible, tomography are performed to identify or reveal corneal abnormalities and irregular astigmatism. I find the measurements provided by the Pentacam (Oculus Optikgeräte), specifically the RMS HOA WE (6 mm) in the Holladay report or the Total Corneal HOA (4 mm) in the cataract preoperative report, to be useful in quantifying irregular astigmatism and HOAs (Figure 2). For example, I would not recommend a diffractive IOL if the RMS HOA WE exceeds 1. Wavefront aberrometers such as the OPD-Scan III (Marco), iTrace (Tracey Technologies), and Pentacam AXL Wave (Oculus Optikgeräte) can also be useful for this purpose and provide additional information about an eye’s optical quality and potential.

Figure 2. Images from the Pentacam Holladay Report show an eye with significant irregular astigmatism and a history of 16-cut RK. Cataract surgery with implantation of an IC-8 Apthera IOL is planned.
I find the following two basic metrics useful, simple to execute, and readily available: the patient’s BSCVA (both present and historical) and their BCVA with a hard contact lens overrefraction. If spectacles adequately corrected a patient’s vision before cataract development, I am confident that the individual has minimal or mostly regular astigmatism and a toric IOL or arcuate/limbal relaxing incisions are likely to be effective. When a patient requires or historically required a rigid gas permeable or scleral contact lens for good quality vision, I assume, until proven otherwise, that irregular astigmatism is present, which limits surgical treatment options.
OVERVIEW OF SEVERAL TREATMENT OPTIONS
Standard monofocal and monofocal plus IOLs. Implantation of these lens types is the most conservative approach to virtually any situation. I consider the spherical aberration of the IOL (most often negative) and try to match it with the corneal spherical aberration (most often positive). Monofocal plus IOLs such as the Tecnis Eyhance (Johnson & Johnson Vision) may offer additional depth of focus compared to a standard monofocal lens with little to no downside. In eyes where achieving good centration of the IOL relative to the visual axis may be challenging, I sometimes favor a spherically neutral IOL such as the SofPort AO (model L161A0, Bausch + Lomb).
Extended depth of focus IOLs. In the presence of corneal abnormalities, extended depth of focus (EDOF) IOLs are less forgiving than a standard monofocal lens but more forgiving than bifocal, trifocal, or combined-technology IOLs. I sometimes implant a Tecnis Symfony OptiBlue IOL (Johnson & Johnson Vision) in eyes with mild corneal irregularity because the lens has a large (1.6-mm) central ring for distance vision and performs well in low-contrast and low-light settings. Nondiffractive EDOF IOLs such as the Clareon Vivity (Alcon) and RayOne EMV (Rayner) work by extending the waveform or strategically inducing spherical aberration. These lenses can be useful when minimizing glare or halos is desired.
Multifocal, trifocal, and combined technology IOLs. I generally avoid these lenses in patients with irregular corneas and/or high amounts of irregular astigmatism because I want to preserve contrast sensitivity and visual quality to the greatest extent possible.
Toric IOLs. Toric versions of all standard and premium IOL options discussed are available. They perform best in eyes with a high amount of regular astigmatism (generally > 0.75 D against the rule or > 1.25 D with the rule) but a low amount of irregular astigmatism. If a patient has a high amount of irregular astigmatism and it is determined that a hard contact lens may be required after surgery for optimal vision, a nontoric IOL may be more appropriate.
Light Adjustable Lens. The Light Adjustable Lens (LAL; RxSight) is virtually as forgiving as a standard monofocal lens, but its postoperative adjustability increases the likelihood of achieving optimal refractive outcomes. Furthermore, when blended vision is targeted and light treatments are performed strategically, the LAL can provide a depth of focus comparable to an EDOF IOL. From my experience, this can be achieved if -0.50 D or more is targeted in the nondominant eye, the light treatment is performed in a positive-to-negative direction (ie, from a hyperopic or plano manifest refraction toward a myopic manifest refraction target), and if the total amount of astigmatic correction is reduced to less than 1.00 D to conserve sufficient macromers for the adjustment of sphere and induction of an EDOF.
The LAL is suitable for patients with mild irregular astigmatism if their BSCVA is (or was) satisfactory. I have had success combining Descemet membrane endothelial keratoplasty and cataract extraction with LAL implantation in patients who have visually significant Fuchs dystrophy and cataract who desire premium outcomes.
The LAL is not my first choice for individuals with significantly aberrated corneas or high amounts of irregular astigmatism, as can be the case in patients with advanced keratoconus or a history of RK involving 16 or more incisions.
Small-aperture IOL. The IC-8 Apthera IOL (Bausch + Lomb) features a small (1.36-mm) central aperture that extends depth of focus, increasing visual acuity at various distances, and normalizes (at least) 1.50 D of corneal astigmatism (both regular or irregular). Currently in my practice, prospective candidates undergo a pilocarpine trial to confirm their comfort with a reduction in light reaching the retina.
The IC-8 Apthera IOL is indicated for implantation in the nondominant eye, with a monofocal IOL placed in the dominant eye. For patients with significant bilateral irregular astigmatism, I implant the lens bilaterally (off-label indication). In such cases, I consider targeting a postoperative refraction of -0.75 D in the dominant eye to provide adequate distance to intermediate visual acuity and targeting a greater amount of myopia in the nondominant eye.
CONCLUSION
Advances in diagnostics and IOL platforms are expanding our ability to offer refractive cataract surgery to patients with irregular corneas and irregular astigmatism. It is important for surgeons to be conservative when dealing with these tough cases, while simultaneously leveraging the latest and greatest technologies. This can allow us to underpromise and overdeliver on results to our patients.
