
Posterior capsular opacification (PCO) results naturally after cataract surgery and can lead to a degradation of visual function. Risks for postoperative PCO include eyes with early cataract onset, high myopia, and ocular inflammation. Inadequate removal of nuclear remnants in the capsular bag during surgery and a diagnosis of diabetes can also increase the risk of PCO. Further, IOL materials and lens designs play a role in PCO formation. Despite preventive measures like the use of lenses designed with a square edge and meticulous polishing of the anterior capsule after IOL implantation, a posterior capsulotomy Nd:YAG laser treatment within 2 to 5 years after cataract surgery is performed in about 20% to 50% of cases.1
ASSOCIATED COMPLICATIONS AND SOLUTIONS
If PCO occurs, the current standard of care is to wait 6 months before performing an Nd:YAG treatment. Complications from PCO, however, including Elsching pearls, capsular folds, fibrosis, Soemmering rings, and subsequent visual loss, halos, and reduced contrast sensitivity can occur. With certain lenses, such as multifocal diffractive and extended depth of focus IOLs, any fibrosis can result in an immediate loss of contrast sensitivity.
Nd:YAG treatments have limitations. There is a steep learning curve, especially for young ophthalmologists. Pitting of the IOL, iatrogenic floaters, macular cystoid edema, and retinal detachment are all concerns.
Alternatively, a novel approach to a posterior capsulotomy is the Premium Refractive Outcome Capsulotomy (PROcap™) technique, which can be performed with the Tango Reflex™ Neo (Lumibird Medical; Figure 1).
Figure 1. The tango reflex neo Nd:YAG laser.
This Nd:YAG laser delivers a brief low-energy laser pulse behind the posterior capsule to create a polygon-shaped capsular opening (Figure 2). Laser pulses are then delivered beneath each angle under tension, extending the posterior capsulotomy and creating symmetrical exposure behind the IOL.
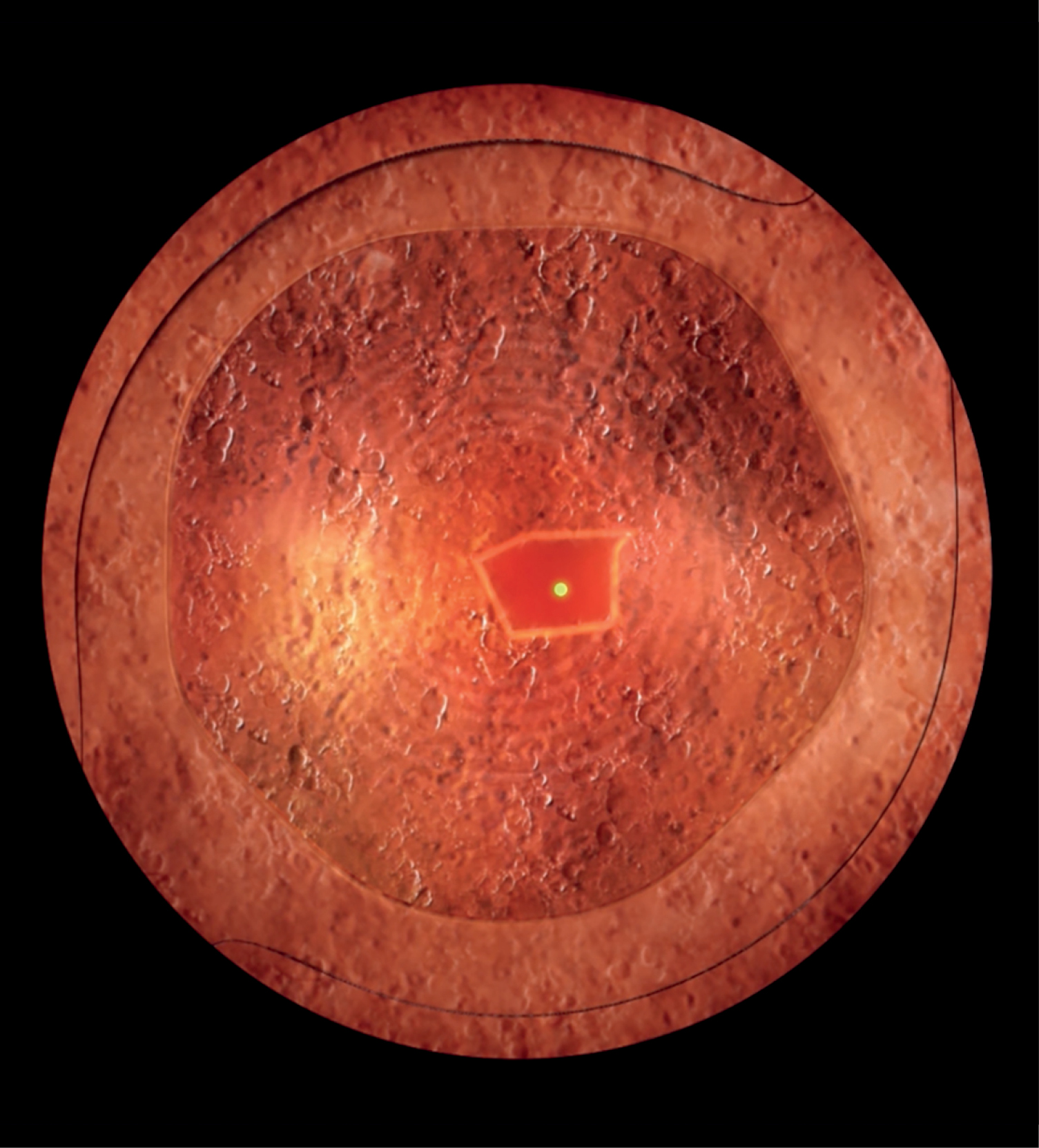
Figure 2. The laser creates a polygonal opening.
The Nd:YAG laser pulse ionizes intraocular matter and causes the rapid growth and decay of a cavitation bubble and its accompanying shockwave moving toward the posterior capsule. With a sufficient posterior offset of up to 2 mm—versus other lasers that allow an offset of less than 500 µm—the collapsing cavitation bubble produces a powerful jet-effect to cleanly dissect tissue.
PROcap™ causes minimal debris and decreases the risk of inadvertent damage to an IOL, such as IOL pitting (Figure 3).
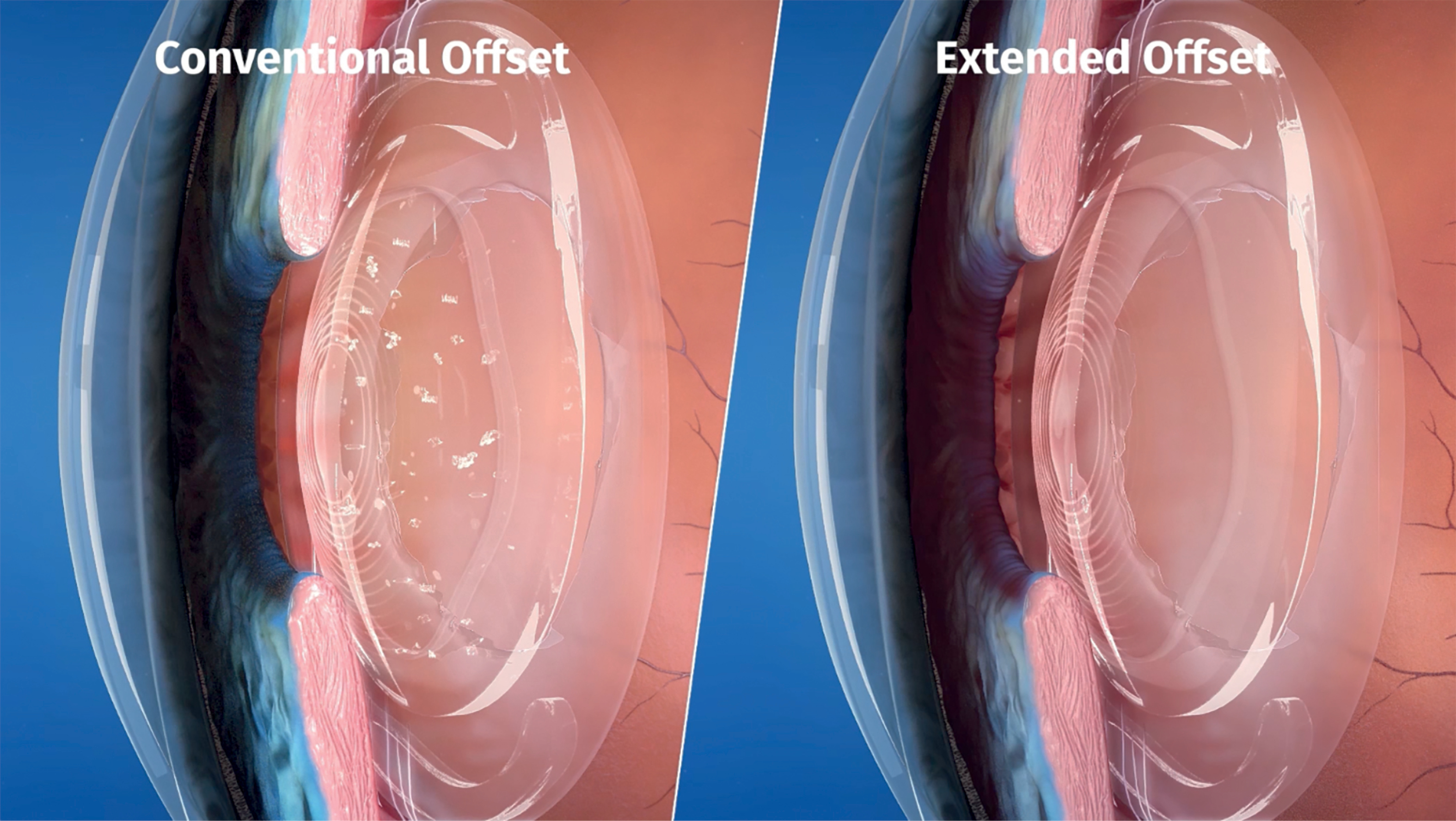
Figure 3. The tango reflex neo Nd:YAG laser has an extended offset compared to other Nd:YAG lasers.
With Imprint™, a dynamic heads-up display incorporated into the binoculars, laser energy can be adjusted easily via the joystick without the surgeon looking away from the slit lamp.
CLINICAL BENEFITS
A survey of 113 cataract surgeons was conducted by Lumibird in 2022 to assess Nd:YAG practice patterns. Half of the respondents created an opening of less than 4 mm, and 79% used a posterior offset. The Tango Reflex™ Neo extends the standard posterior offset to 2 mm, enhancing the precision of the procedure.
The second-generation Tango Reflex™ Neo incorporates titratable, true-coaxial illumination (TCI) technology, bringing visual focus, target illumination, and laser treatment beams into alignment, in one optical plane, providing a full red reflex from the retina. TCI technology provides spatial integrity and excellent contrast of important ocular structures (Figure 4). This ensures accurate targeting, minimizing the risk of complications.
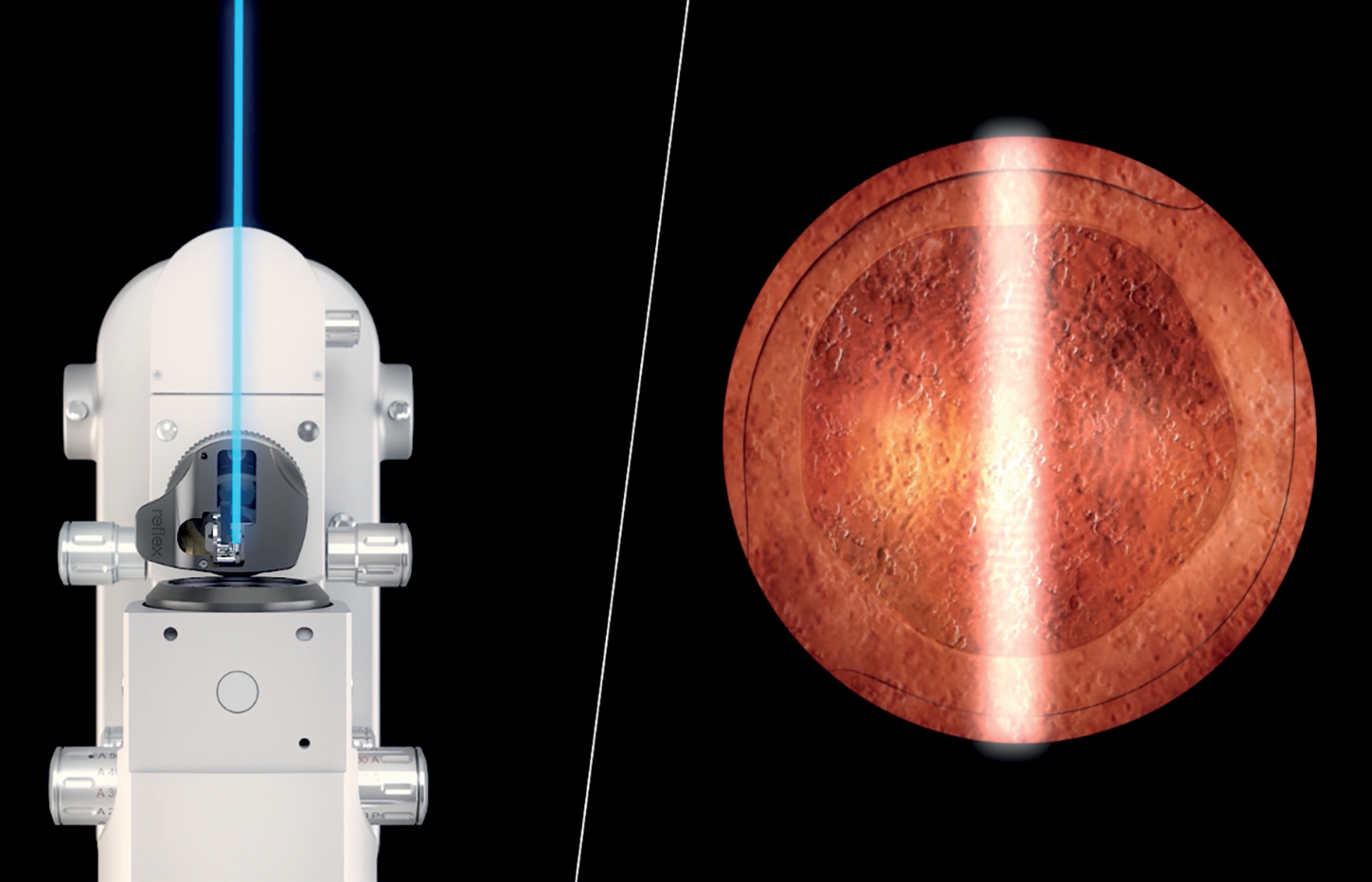
Figure 4. TCI technology produces excellent contrast of important ocular structures.
Figure 4 courtesy of Karl Brasse, MD
The laser can be delivered at a frequency of four times per second with consistent optical breakdown at very low energy.
With a conventional Nd:YAG capsulotomy, typical posterior offsets used in practice are below 300 µm. The laser-induced cavitation bubble produces a mechanical shockwave, which is the principal mechanism for tissue disruption (Figure 5).
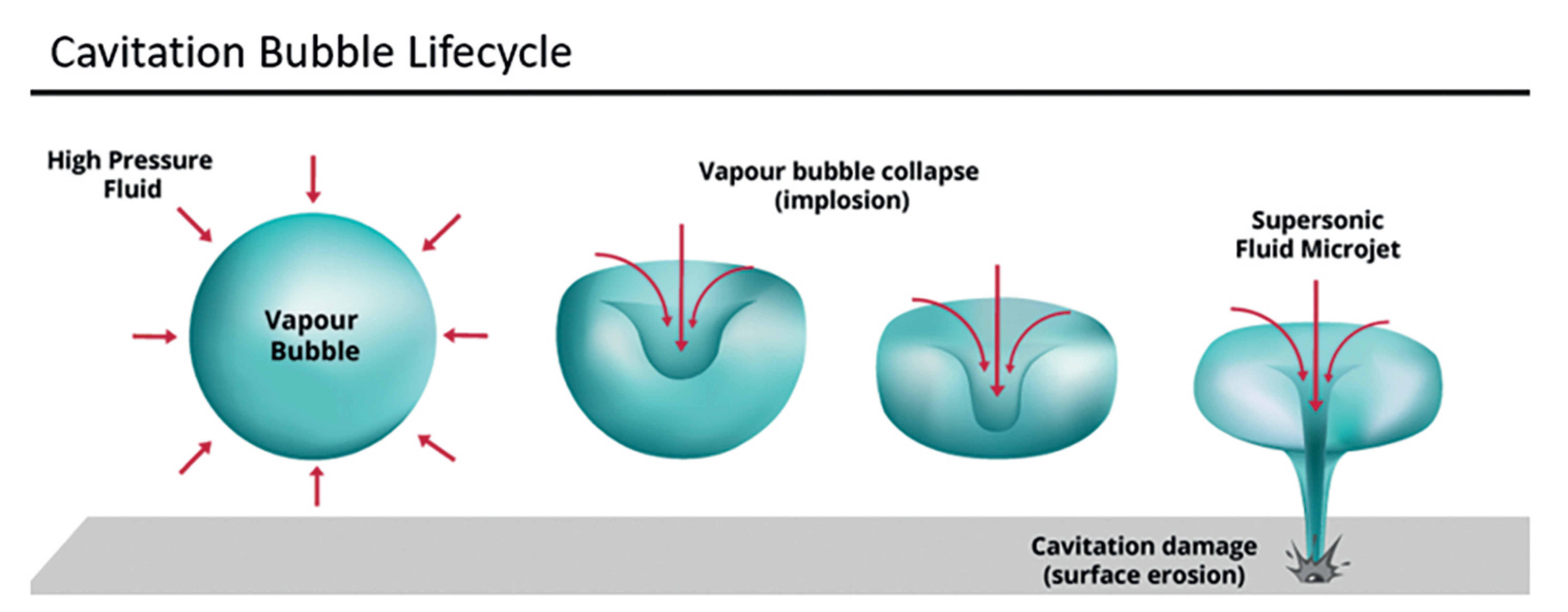
Figure 5. Cavitation bubble lifecycle.
At more than 1,000 µm, the laser-induced cavitation bubble behaves differently, completing its natural lifecycle and collapsing on itself when overcome by surrounding vitreous pressure. Due to the proximity of a solid boundary—the IOL—the cavitation bubble collapses asymmetrically, propelling a high-speed liquid jet from the bubble toward the solid boundary.
This “jet effect” has destructive properties, efficiently cutting the posterior capsule membrane.
It is the liquid jet and not the propagating mechanical wave that causes disruption, and because of the distance involved, the IOL is rendered completely safe from harmful pitting. This allows the procedure to be started universally from the center, avoiding the common trade-off of a large iatrogenic floater created by circular techniques.
PROcap™ makes it feasible to produce adequately sized openings, exposing the full functional benefit of premium IOLs, protecting the lens and avoiding iatrogenic floaters, and overcoming the three most common problems associated with the procedure today.
CONCLUSION
Even with preventive methods like anterior and posterior capsular polishing and novel IOL materials and designs, there is no single way to completely avoid PCO formation. We are on a quest for effective and safe treatments to preserve the eye from floating bodies, maintain IOL centration, limit energy dispersion, and protect against IOL damage. PROcap™ is a promising technique to treat PCO and reduce floaters when performed with careful focus and energy adjustment.
As the premium IOL market grows, so does the need for a simple, safe, and effective solution to the problem of PCO. In my clinical experience, PROcap™ is emerging as a revolutionary treatment for PCO. It offers enhanced safety, precision, and outcomes for Nd:YAG laser treatments. The fusion of Lumibird Medical’s innovative technology with surgeons’ clinical expertise brings us one step closer to overcoming the challenges posed by PCO and improving the overall patient experience.
1. Sinha R, Shekhar H, Sharma N, Titiyal JS, Vajpayee RB. Posterior capsular opacification: a review. In J Ophthalmol. 2013;61(7):371-376.

