
Introduction
Maintaining anterior chamber stability is a critical factor for successful cataract surgery. Anterior chamber stability is associated with variable inflow and outflow rates that affect intraocular pressure (IOP).1,2 Gravity-based fluidics has been a standard in cataract surgery for decades. However, the anterior chamber stability remained a subject for improvement.3 The Centurion® Vision System with Active Fluidics® (Alcon) was the first technology to replace traditional gravity-based phacoemulsification to respond to any changes in IOP. The system compresses the bag with balanced salt solution (BSS), and the more the surgeon removes fluid from the anterior chamber, the more it compresses the bag, replenishing the volume that was removed.4 Thus, irrigation is adapted to aspiration at each step of the cataract surgery procedure, and pressure in the anterior chamber is maintained at a constant value. Infusion pressure control provided by Active Fluidics® improves anterior chamber stability and enables the use of lower IOPs during cataract surgery.5,6 The Centurion® Vision System with Active Fluidics® raised the predictability of phacoemulsification to new heights.2 Then Active Fluidics® technology was upgraded with the Active Sentry® Handpiece (Alcon) which contains a built-in pressure sensor that reacts in real time to enhance performance and hasten response to surge.7 One of the great challenges to safe and efficient cataract surgery is the occlusion break surge phenomenon: a partial or complete collapse of the anterior chamber that can happen during phacoemulsification.8 Because surges occur on a millisecond timescale, they are too quick for human intervention. This sudden reduction in aqueous volume can traumatize the cornea, iris, posterior capsule, or zonular fibers.9,10 The Centurion® Vision System with Active Fluidics® contains a sensor near the cassette while the Active Sentry® Handpiece measures IOP very near the anterior chamber, minimizing the delay in adjusting the fluidics. Centurion® Vision System with Active Sentry® includes QuickValve™ technology, a redesigned valve that is responsive to the fluidics change. Thus, the Centurion® system with Active Sentry® compensates for an occlusion break surge by detecting its onset through a handpiece with a built-in pressure sensor and partially venting the stored vacuum before the volume is demanded by the anterior chamber to minimize the occlusion break surge and ensure anterior chamber stability.5,9 Finally, the Active Sentry® software ensures a seamless process (Figure 1).4
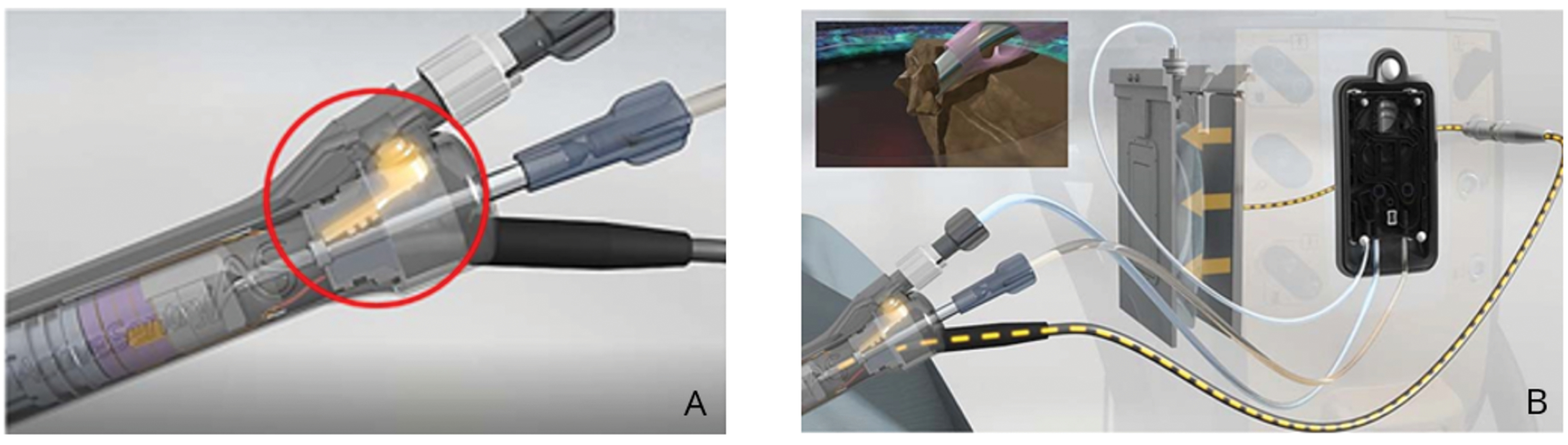
Figure 1. The Active Sentry® Handpiece features a built-in pressure sensor that reacts in real time (A). Active Sentry® communicates with hardware and software to compensate for changes in the anterior chamber (B). When occlusion happens, the system detects it and signals for a pressure adjustment to the BSS bag.
Active Sentry® performance in an experimental and a clinical environment
The Active Sentry® technology allows faster mitigation of surge response, ensuring anterior chamber stability, which has been shown in several experimental studies.5,9,11,12 The transient changes in anterior chamber volume after occlusion break have been tested using spring eye model—simulated anterior chamber of the human eye.13 This experimental study analyzed the volumetric occlusion break surge responses of 3 phacoemulsification systems: Infiniti®, Centurion® Active Fluidics®, and Centurion® with Active Sentry® at different vacuum limits and target IOPs of 30, 55 and 80 mm Hg. The authors highlighted impressive improvements in fluidics technology with Centurion® Active Sentry®, allowing reduced surge volumes. The surge volumes under the most strenuous target IOP of 30 mm Hg with Active Sentry® were comparable to those of the base Centurion® system under the conventional target IOP of 80 mm Hg, regardless of the vacuum limit. Thus, the surgeon can work at IOPs that are comfortable for the patient and closer to physiological levels without risking sudden chamber collapse.9
In a published study,11 the authors used the slit side view (SSV) method to visually evaluate fluid flow within the anterior chamber during surgery, as it clearly provides good volumetric view of the chamber.14 Anterior chamber depth (ACD) changes during occlusion break were observed using the SSV method, recorded, and analyzed for Centurion with Ozil handpiece (Alcon; group 1), Centurion with Active Sentry (group 2), and gravity-based phacoemulsification systems (Infiniti Vision System and Constellation Vision System [both Alcon]—groups 3 and 4, respectively). The percentage change in the ACD after the occlusion break (ACD change ratio) was calculated for each group. The ACD change ratios in groups 1, 2, 3, and 4 were 17.5% ± 3.9%, 7.3% ± 1.2%, 35.7% ± 9.5%, and 74.1% ± 7.7%, respectively. There was a significant difference among the four groups and between groups 1 and 2 (Figure 2).11
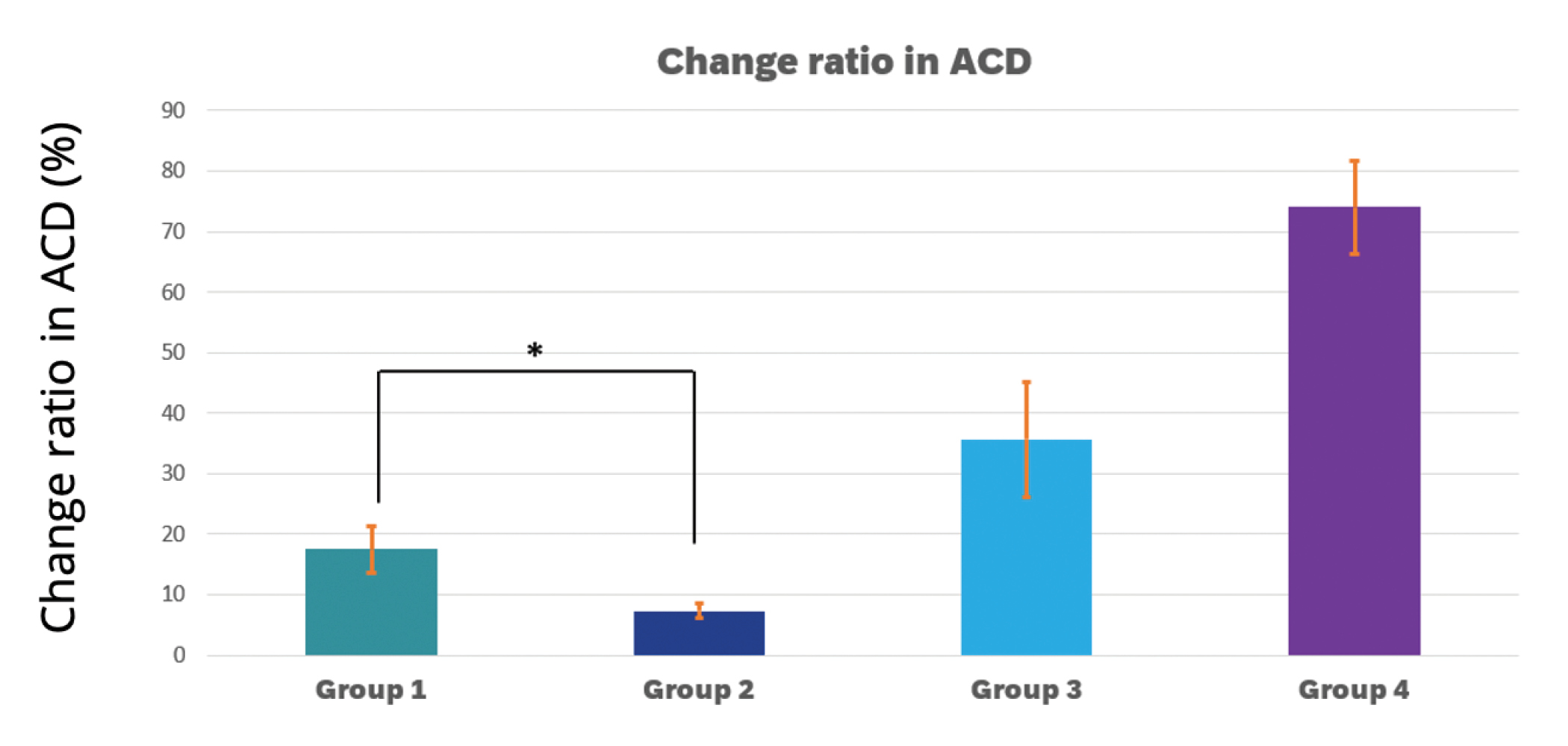
Figure 2. Change ratio in ACD. P < 0.05, Kruskal-Wallis test; *P < 0.05, Mann-Whitney U test. The ACD change ratios in groups 1, 2, 3, and 4 were 17.5% ± 3.9%, 7.3% ± 1.2%, 35.7% ± 9.5%, and 74.1% ± 7.7%, respectively.
ACD: anterior chamber depth

The number of publications focusing on Active Sentry clinical data are increasing. The results of 200 eyes of 129 patients that were operated on for cataracts using Centurion Active Sentry (n = 100) or Centurion Ozil (n = 100) have been evaluated in a retrospective study. The Active Sentry Handpiece allowed the surgeon to significantly reduce IOP and substantially eliminate post-occlusion waves. Upon the use of the Centurion Ozil Handpiece, average perioperative IOP was 65 mm Hg. Upon the use of the Active Sentry Handpieces, it was possible to reduce perioperative IOP safely to 46 mm Hg (P < 0.005). The study demonstrated a statistically significant reduction of the average values of Cumulated Dissipated Energy (CDE) (4.78 [SD ± 2.83] vs. 6.11 [SD ± 3.26], P = 0.002) and total ultrasound time (30.1 seconds [SD ± 10.5] vs. 42.2 seconds [SD ± 8.9], P = 0.003) in the Active Sentry group in comparison with the Centurion Ozil group.15 The study by Sabur and Unsal16 showed that CDE and torsional amplitude measured in the Active Sentry group were significantly lower than those of the Centurion Ozil group (8.8 ± 3.9, 10.4 ± 4.2, P = 0.016 and 51.2 ± 13.3, 65.2 ± 9.3, P = 0.000, respectively).
The experimental data showing better anterior chamber stability5,9,11,12 with Active Sentry are supported by clinical data.7 Moreover, clinical data show that the Active Sentry technology allows cataract surgeons to operate at more physiological IOP levels without compromising the anterior chamber stability.7
The recent studies provide more data on the Active Sentry intra-operational performance and clinical benefits for patients.17,18 The SASCA study (Study of Active Sentry in CAtaract surgery) was a multicentral prospective clinical study conducted at Université Paris Cité, Hôpital Cochin, and four other clinical sites in France. We analyzed 1432 cataract surgery procedures comparing Centurion Active Sentry (n = 800) and Centurion with a traditional handpiece (non-Active Sentry) (n = 632). The main outcome measured was the CDE used during phacoemulsification. Secondary outcome measures were the total procedure duration, the total ultrasound time, and the frequency of adverse events. The mean CDE was significantly lower with Active Sentry (8.0 ± 7.19) than without (9.3 ± 8.47) [P = 0.0001]. The duration of surgery and the total ultrasound time were shorter for the Active Sentry group than for non-Active Sentry. The duration of surgery was (9.8 ± 4.47 and 11.0 ± 9.22 minutes, P = 0.0002), and the total ultrasound time was (55.7 ± 38.66 and 63.6 ± 37.83 seconds, P < 0.0001) for Active Sentry and non-Active Sentry, respectively. No posterior capsule rupture during the phacoemulsification was recorded in either group. The SASCA study results demonstrated that phacoemulsification with Active Sentry significantly reduced the amount of energy used during the procedures and shortened their duration. We hypothesize that the higher efficiency of the procedures with the Active Sentry Handpiece could be explained by surgeons’ higher confidence in anterior chamber stability when using the phaco handpiece to prevent the surges. Thus, the surgeons emulsified the lens quicker.
Another recent study was conducted to investigate the effect of near-physiologic IOP (20 mm Hg) versus high IOP (50 mm Hg) cataract surgery, performed with Active Sentry, on the cornea.18 The study showed a significantly higher protection rate of endothelial cell density and less corneal edema with near-physiologic IOP versus high IOP (Figure 3).
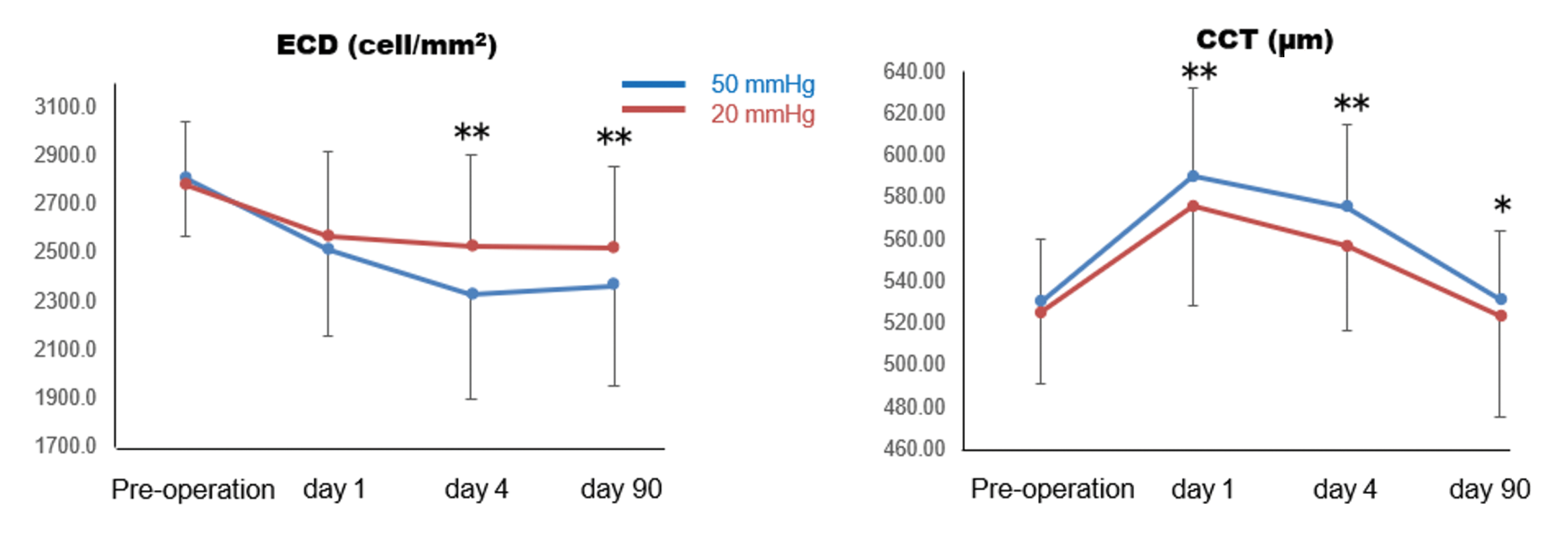
Figure 3. Corneal parameter changes. *P < 0.05, **P < 0.01 two-way repeated measure ANOVA with post-hoc Bonferroni test.
Conclusions
Phacoemulsification devices and technologies have been continuously developing to increase the effectiveness and to reduce the potential risks of the cataract surgery procedure. The Active Fluidics technology broke new ground in phacoemulsification technologies, now enhanced by the Active Sentry Handpiece. It allows surgeons to operate with confidence in anterior chamber stability, which is not compromising at a range of intraoperative IOP levels including near-physiologic IOP.
© 2024 Alcon Inc. 01/24 GLB/IMG-CNT-2400001
The views and opinions expressed in this content may not necessarily represent those of Bryn Mawr Communications or Cataract & Refractive Surgery Today Global.
1. Solomon KD, et al. Clinical study using a new phacoemulsification system with surgical intraocular pressure control. J Cataract Refract Surg 2016;42:542–549.
2. Cyril D, et al. Comparison of two phacoemulsification system handpieces: prospective randomized comparative study. J Cataract Refract Surg. 2022;48:328–333.
3. Nicoli CM, et al. Experimental anterior chamber maintenance in active versus passive phacoemulsification fluidics systems. J Cataract Refract Surg. 2016;42:157–162.
4. Centurion® Vision System Operator’s Manual.
5. Miller KM, Dyk DW, Yalamanchili S. Experimental study of occlusion break surge volume in 3 different phacoemulsification systems. J Cataract Refract Surg. 2021;47:1466-1472.
6. Chang JS, Ng JC, Chan VK, Law AK. Cataract surgery with a new fluidics control phacoemulsification system in nanophthalmic eyes. Case Rep Ophthalmol. 2016;7:218–226.
7. Beres H, de Ortueta D, Buehner B, Scharioth GB. Does low infusion pressure microincision cataract surgery (LIPMICS) reduce frequency of post-occlusion breaks? Rom J Ophth. 2022;66(2):135-139.
8. Han, Y. K. (2014). Fluidics of phacoemulsification systems. In Cataract Surgery: Maximizing Outcomes Through Research (pp. 113-126). Springer Japan. https://doi.org/10.1007/978-4-431-54538-5_10
9. Thorne A, Dyk DW, Fanney D, Miller KM. Phacoemulsifier occlusion break surge volume reduction. J Cataract Refract Surg. 2018;44:1491-1496.
10. Sharif-Kashani P, Fanney D, Injev V. Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems. BMC Ophthalmol. 2014;14:96. Available at: http://www.biomedcentral.com/content/pdf/1471-2415-14-96.pdf.
11. Suzuki H, Igarashi T, Takahashi H. Effect of a new phacoemulsification and aspiration handpiece on anterior chamber stability. J Cataract Refract Surg. 2023;49:91–96.
12. Vasavada V, Vasavada AR, Vasavada VA, Vasavada SA, Bhojwani D. Real-time dynamic changes in intraocular pressure after occlusion break: comparing 2 phacoemulsification systems. J Cataract Refract Surg. 2021;47:1205-1209.
13. Dyk DW, Miller KM. Mechanical model of human eye compliance for volumetric occlusion break surge measurements. J Cataract Refract Surg. 2018;44:231-236.
14. Suzuki H, Igarashi T, Shiwa T, Takahashi H. A novel “slit side view” method to evaluate fluid dynamics during phacoemulsification. Hindawi Journal of Ophthalmology. Volume 2018, Article ID 5027238.
15. Jirásková N, Stepanov A. Our experience with active sentry and centurion ozil handpieces. Cesk Slov Oftalmol. 2021;77:18-21.
16. Sabur H, Unsal U. The efficacy and safety profile of cataract procedures performed with a sensorembedded handpiece and a new hybrid phaco tip. Eur J Ophth. 2022;32(6):3438-3443.
17. Brézin AP, Monnet D, Lignereux F, Rozot P, Jilet L, Abdoul H. Impact of a handpiece with a built-in fluidics pressure sensor on phacoemulsification: a multicentre prospective comparative study. BMJ Open Ophth 2023;8:e001431. doi:10.1136/bmjophth-2023-001431.
18. Kokubun T, et al. Verification for the usefulness of normal tension cataract surgery. The 126th Annual Meeting of the Japanese Ophthalmological Society, April 2022.

Caution: Federal (USA) law restricts this device to sale by, or on the order of, a physician.
As part of a properly maintained surgical environment, it is recommended that a backup IOL injector be made available in the event the AutoSert® IOL Injector Handpiece does not perform as expected.
Indication: The CENTURION® Vision system is indicated for emulsification, separation, irrigation, and aspiration of cataracts, residual cortical material and lens epithelial cells, vitreous aspiration and cutting associated with anterior vitrectomy, bipolar coagulation, and intraocular lens injection. The AutoSert® IOL Injector Handpiece is intended to deliver qualified AcrySof® intraocular lenses into the eye following cataract removal.
The AutoSert® IOL Injector Handpiece achieves the functionality of injection of intraocular lenses. The AutoSert® IOL Injector Handpiece is indicated for use with the AcrySof® lenses SN6OWF, SN6AD1, SN6AT3 through SN6AT9, as well as approved AcrySof® lenses that are specifically indicated for use with this inserter, as indicated in the approved labeling of those lenses.
Warnings: Appropriate use of CENTURION® Vision System parameters and accessories is important for successful procedures. Use of low vacuum limits, low flow rates, low bottle heights, high power settings, extended power usage, power usage during occlusion conditions (beeping tones), failure to sufficiently aspirate viscoelastic prior to using power, excessively tight incisions, and combinations of the above actions may result in significant temperature increases at incision site and inside the eye, and lead to severe thermal eye tissue damage.
Good clinical practice dictates the testing for adequate irrigation and aspiration flow prior to entering the eye. Ensure that tubings are not occluded or pinched during any phase of operation.
The consumables used in conjunction with ALCON® instrument products constitute a complete surgical system. Use of consumables and handpieces other than those manufactured by Alcon may affect system performance and create potential hazards.
AEs/Complications: Inadvertent actuation of Prime or Tune while a handpiece is in the eye can create a hazardous condition that may result in patient injury. During any ultrasonic procedure, metal particles may result from inadvertent touching of the ultrasonic tip with a second instrument. Another potential source of metal particles resulting from any ultrasonic handpiece may be the result of ultrasonic energy causing micro abrasion of the ultrasonic tip.
ATTENTION: Refer to the Directions for Use for the accessories/consumables and Operator’s Manual for a complete listing of indications, warnings, cautions and notes.
