
HISTORICAL OVERVIEW
Ronald R. Krueger, MD: Modern refractive surgery started with radial keratotomy in the 1970s,1,2 but the subspecialty was truly born with the introduction of the excimer laser. PRK became widely accepted in the ‘90s, quickly followed by LASIK.3,4 The evolution of refractive surgery continued with the introduction of femtosecond lasers for creating flaps5 and customized ablation profiles and personalized treatments, bringing us to the current technologies that we have today.
LASIK is the most frequently performed elective procedure in all of refractive surgery.6,7 Long-term studies indicate good stability for more than 10 years and high patient satisfaction.8 Overall, nowadays there is a low risk of complications with LASIK,8 due in part to newer diagnostic tools and refinements in ablation profiles.
Over the years, we have learned how corneal ablation profiles can be designed to prevent the induction of spherical aberration—one of the greatest aberrations created with LASIK—and treat higher-order aberrations (HOAs) like coma. Personalization and customization of the ablation profile has become a significant advancement, bringing us to the newest procedure, which is wavelight plus (Alcon). Before we talk about wavelight plus, Dr. Kanellopoulos, please give us a brief overview of customization in laser vision correction.
A. John Kanellopoulos, MD: The first standard ablation profile was designed to correct myopia and soon after myopic astigmatism. They ignored the corneal asphericity, and initially there were some issues, including centration during ablation delivery since it was set manually and decentrations along with pupillary diameter, that induced frustrating visual quality issues when spherical aberration was induced. When asphericity-adjusted (ie, wavefront-optimized) profiles and improved dynamic tracking were introduced, the laser could then better center the changes in corneal curvature and induce less spherical aberration. These treatments compensate for cosine effects, provided a more prolate corneal shape, and avoided inducing spherical aberration. Later advancements allowed the correction of coma, trefoil, and other aberrations in the total optical system. Other wavefront-optimized ablations such as Custom Q allow customization of the asphericity.9
Wavefront-guided ablations, on the other hand, are based on preoperative whole eye aberrometry. These treatments correct sphere and cylinder but also attempt to improve HOAs. Although effective, wavefront-guided ablations precompensate only for rotationally symmetrical aberrations, they do not provide information from the specific optical properties of the eye, and do not consider individual corneal properties.
Refractive surgeons, and our team in particular, continued to push the boundaries to improve outcomes, bringing us to the current era of tomography-guided and ray-tracing ablations. Now, we're able to treat some of the intrinsic aberrations of the human eye. We can recenter the cornea to each patient’s individual visual axis, correcting most of the HOAs, mainly coma.
Our appetite for customized ablations has grown in parallel to the great visual function outcomes patients experience. Tomography-guided ablations were originally designed to treat irregular corneas but became a mainstay for naive myopic eyes. It has been a tremendous tool throughout the years and, I think, they have become the strongest segue to ray tracing because we learned through clinical application that even healthy eyes have HOA—mainly corneal—that we can improve. We're at a very good point in the history of refractive surgery.
Dr. Krueger: What is so unique about wavelight plus–guided treatments?
Dr. Kanellopoulos: This is a new concept allowing us to move away from using extrapolated outcomes data when analyzing imaging of the cornea and wavefront from several diagnostic devices. With the wavelight plus, we can now use a single device to measure the actual dimensions of an eye with great accuracy; we can then design a 3D eye model for an individual eye by tracing 2,000 rays from the objective measuring device up to the lens of the eye and then backward from the retina through the lens of the eye (Figure 1). It uses a personalized ametropic eye model, considering all refracting surfaces of the eye and their geometrical location within an individual eye instead of relying on the Gullstrand model.9 It also includes a fourth calculated component, which is tilt between the lenticular and the cornea systems. The same device also captures Scheimpflug tomography and Hartmann-Shack wavefront images. Now, we're seeing not only cornea-based aberrations but also tilt and other aberrations in the eye. This is all done automatically.
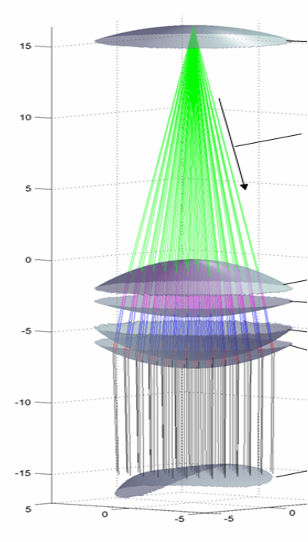
Figure 1. A 3D eye mode is created with the wavelight plus platform.
Dr. Krueger: We have come back full circle with wavelight plus. It’s a wavefront-guided approach with tomography and biometry, but it takes us to the next level because treatment is more personalized than ever before.
Dr. Kanellopoulos: That’s right. The difficulties with wavefront, historically, are it’s a dynamic measurement with significant variability and that it can be measured only through the pupil aperture by definition. The average cornea is 12 mm in diameter; it offers a much larger refractive surface for imaging. Tomography-guided treatments also provide more reproducible measurements besides the wider assessment of corneal optics to a 9-mm diameter. Researchers started investigating how can we combine the two; wavefront plus offers us a combination of both wavefront- and tomography-guided strategies.
INTRODUCTION TO WAVELIGHT PLUS
Dr. Krueger: Dr. Cummings, how do you introduce the concept of wavelight plus to patients?
Arthur B. Cummings, MB ChB, FCS(SA), MMed(Ophth), FRCSEd, FWCRS: One might think it is a complicated subject for patients to grasp, but in fact it's very straightforward when the explanation is simplified for them.9
Generally, wavefront-guided, tomography-guided, and asphericity-guided LASIK ablation profiles are all designed to treat Gullstrand's eye model, which is an eye that is 24 mm long and has a corneal curvature of 43.00 D. With wavelight plus, however, the laser designs an ablation profile for a patient’s individual eye rather than Gullstrand’s model. If the eye happens to be 26.5 mm long and the cornea is 40.00 D, the wavelight plus technology creates a model based on the wavefront, biometry, and tomography measurements of that specific eye.9
A treatment profile is generated, applied to the virtual eye model, and tested by directing light rays through the treated virtual cornea. If these light rays converge on the macula, the ray tracing is ideal. Most times, however, the rays do not all converge on the macula precisely. The rays that have missed the macula are ray traced back toward the cornea and modifications are made to ensure that the cornea is directing all the rays to the macula. This process is repeated or iterated until all the incoming rays on the virtual eye model (ie, the avatar of the human eye) meet perfectly at the macula. I've yet to meet a patient who couldn't understand the principle of this personalization and see the value of such a powerful technology.
In the initial clinical trials, ray tracing showed the most potential for treating longer eyes and eyes that differed significantly from Gullstrand’s eye model (ie, eyes not 24 mm long and not with 43.00 D corneal curvature),10,11 but more recent trials have shown that it provides superior results in any eye, irrespective of whether it's close to a Gullstrand model or not.12 Now, with wavelight plus, we can offer patients the ultimate personalization by using their own eye as an avatar for treatment planning.
TREATMENT DECISION-MAKING AND PLANNING
Dr. Krueger: Dr. Bala, how do you decide when to use a tomography-guided correction versus a wavefront-guided correction versus, now, a wavelight plus correction?
Chandra Bala, MBBS, PhD, FRANZCO: It is tantalizing to be able to correct wavefront aberrations. One thing I like to remember is that we cannot change the light that comes past the cornea and into the eye. But what we can change is the light when it hits the cornea. This is what a tomography-guided treatment does. But to change the light even slightly, we must know what's going to happen inside the eye. We now have a complex mathematical system using ray tracing that accounts for the rays of light passing downstream, and for the first time, we can change the angle of incidence of light at the cornea and know whether it'll hit the fovea or scatter. I think I will be using ray tracing more and more because it’s the next big step in our ability to give patients excellent visual outcomes.
Dr. Krueger: Dr. Khoramnia, you have performed tomography-guided LASIK for quite some time with success. What factors come to mind when you think of using a wavelight plus ray-tracing treatment?
Ramin Khoramnia, MD, PhD: Femtosecond LASIK is effective, but the visual acuity results that we obtained in the wavelight plus clinical trials were much better than what was achieved with traditional laser treatments.13 For that reason, I feel confident switching to wavelight plus. It makes very little sense for me to use other treatment options when wavelight plus can do better. In the past, we spent a lot of time looking at all the images and choosing the right ones for the laser treatment (eg, Contoura, Alcon). With wavelight plus, however, all the data is already in the laser system for us.
Dr. Krueger: Can you walk us through the planning steps for a wavelight plus treatment using Sightmap?
Dr. Bala: Sightmap is a single diagnostic device that incorporates biometry, corneal tomography, and ocular wavefront (Figure 2).9 It’s very easy and simple to do, and all measurements are completed in less than 8 minutes after a subjective refraction is performed. The wavefront is taken and converted into a mathematical eye model that incorporates the tomography, axial length, and wavefront. This eyevatar is then used to generate a digital treatment plan, optimized without any input from the surgeon. It offers great possible accuracy to improve the refractive predictability of laser vision correction.11

Figure 2. Sightmap, a single diagnostic device that incorporates biometry, corneal tomography, and ocular wavefront.
Sightmap imaging has multiple components, including a wavefront, auto refraction, subjective refraction, axial length measurements, tomography, and iris registration (Figure 3).9 Additional measurements can be achieved and aligned to the corneal vertex. The data populates wirelessly, and there is no need for a patient-specific nomogram adjustment.
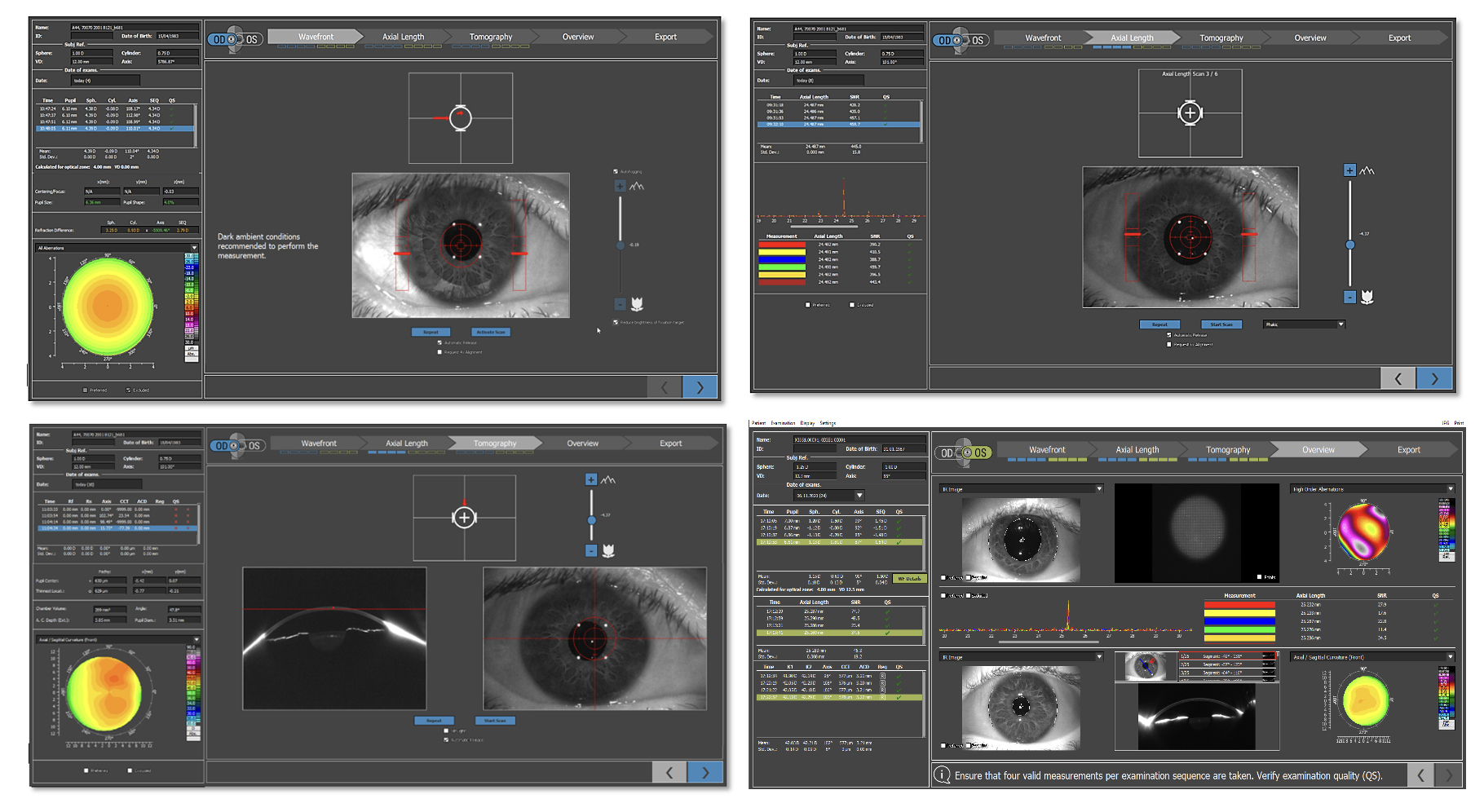
Figure 3. Sightmap provides multiple measurements including a wavefront, auto refraction, subjective refraction, axial length measurements, tomography, and iris registration.
An automatic planning process increases workflow efficiency. To me, an all-in-one system like wavelight plus with Sightmap is invaluable. It also takes up much less real estate in the office. Patients used to have to move between six different devices. Now, they sit at just one. This also cuts down on measurement variability by keeping the measurements aligned and overall the reduced time may reduce dryness, which can produce unstable data.
Dr. Krueger: Dr. Khoramnia, how easy has it been for you to capture data with the Sightmap? In the FDA trial, we had additional steps to follow the study protocol, but in a post-market environment, how easy is it?
Dr. Khoramnia: Like with any new device, training is crucial. Once the staff is trained, the consistency of measurements with this all-in-one device is a great step forward compared to synthesizing data from multiple devices. Also, it is important to remember that traditional femtosecond LASIK treatments require a subjective refraction. It's much more difficult to train somebody to do an accurate subjective refraction than it is to use the Sightmap device. I really think this device will make patient selection and all the prerequisite measurements much easier.
In the past, I had had to double check the subjective refraction, corneal thickness, and other parameters that the staff had entered into the laser. None of this is necessary with Sightmap. I would say that the main benefit of the procedure is that it handles treatment selection for the surgeon and saves a lot of time in the OR.
Dr. Krueger: The bulk of what I do in the United States, where I practice, is tomography-guided treatments. I am excited but also curious about the transition to wavelight plus once it becomes commercially available.
Dr. Bala: I was, too. Now, I use wavelight plus in 95% of cases. In the other 5%, the pupil is too small to obtain appropriate wavefront data.
Dr. Kanellopoulos: The measurements with wavelight plus are done within seconds, and they are just as accurate than measurements with other devices, even in irregular corneas. Additionally, wavelight plus includes automatic and accurate correction of tilt. It’s a no brainer for me to use this procedure over others.
Dr. Krueger: Planning software like Phorcides Analytic Engine (Phorcides) helps simplify preoperative planning, but wavelight plus makes it even simpler.
Dr. Khoramnia: This is one of the real benefits of wavelight plus. If you install the system in four different practices, in my opinion, the outcomes should be equal. With other treatment options, however, it also depends on the physician. Do they really understand which images they should use for the planning? The Sightmap is not dependent on physician selection, and I think that this will help us to get better results throughout all the practices where the device is being used.
Dr. Krueger: How do you decide between wavelight plus and other procedures such as lenticule extraction?
Dr. Khoramnia: Personalization is key. Lenticular extraction can provide excellent results. Traditional femtosecond LASIK can provide excellent results. But, the results achieved with wavelight plus are far more impressive than what we have seen with any procedure in the past. There is therefore very little reason for me not to provide wavelight plus to my patients. Why should I do a lenticular procedure where I get good results when I can get better results with wavelight plus?13 For higher corrections, phakic IOLs can play an important role, but for lower corrections in eyes with a normal cornea, wavelight plus is the way to go.
Dr. Krueger: Dr. Bala, you do phakic IOL implantation. How high do you go with wavelight plus before you start considering an ICL?
Dr. Bala: I've gone as high as -8.00 D depending on the cornea and residual stromal bed. And patients can get good vision with lenticular extraction, but it is not personalized like wavelight plus is.
Dr. Krueger: Dr. Cummings, in your experience, how does the wavelight plus treatment compare to the ICL procedure and lenticule extraction?
Dr. Cummings: With some laser systems, you start to reach the upper limit for laser vision correction at about -6.00 to -7.00 D of myopia. Above this range, many surgeons may decide to proceed with phakic IOL implantation because patients have a greater chance of achieving a superior quality of vision. With the wavelight plus profile, however, the treatment range is much more expansive because it personalizes the ablation profile based on the patient’s individual cornea and ocular optics. In the early clinical trial for wavelight plus, patients’ quality of vision was excellent up to -11.00 D of myopia.14
Corneal biomechanics is also a consideration when selecting the best procedure. Traditionally, PRK is considered to leave the cornea biomechanically stronger than LASIK because the treatment doesn’t penetrate the cornea as deeply, and it avoids cutting corneal fibers.15 LASIK, on the other hand, requires a flap of about 110 µm with a sidecut before the stroma is ablated. With a -4.00 D treatment, a 60-µm ablation is required. When lenticule extraction (KLEx) became an option, the thought was that the procedure might be as biomechanically sound as PRK.16
The key message here is this: Whether the selected procedure is lenticule extraction, LASIK, or PRK, the surgeon must make sure preoperatively with good diagnostic testing that these patients have good corneal integrity.
TREATMENT PROCESS
Dr. Krueger: Dr. Khoramnia, can you walk us through the treatment process with wavelight plus?
Dr. Khoramnia: Wavelight plus is truly the first tailored refractive treatment that considers each patient’s unique optical system. According to the manufacturer, the treatment can be used for up to -11.00 D of sphere and -4.50 D of cylinder.9 It includes a pre-compensation algorithm to account for laser efficiency loss, epithelial remodeling and healing, and biomechanical response for non-symmetrical and symmetric aberrations.9
Dr. Krueger: The built-in pre-compensation is crucial. The wounds are still healing, the epithelium is still thickening after surgery, and the initial result may not be quite as sharp until the eye heals. What is your experience with early versus late outcomes?
Dr. Kanellopoulos: We’ve done extensive research into epithelial remodeling after laser vision correction.17,18 The pattern of remodeling depends on the dioptric power being corrected, but before wavelight plus it was not accounted for. It is very admirable that these patterns are included in the calculations that are done by the wavelight plus software because the corneal epithelium is different in a -2.00 D myope than in a -4.00 D myope and a -6.00 D myope. The software also has the potential for a biomechanical input as well.
Dr. Krueger: In the early tomography-guided studies, patients had great results at 3 months, but at 1 year they got even better.13 The cornea might have continued to improve, along with dryness, but I think there is also some element of neural adaptation involved.
Vision is a complex neurological system. I like the idea of saying to patients, ‘Your final refraction will compensate for the epithelium and corneal biomechanics because ultimately we don’t want you to lose that wow effect over time.’
Dr. Bala: The pre-compensation for epithelial healing with wavelight plus is data-driven. This provides a more stable and consistent response in every eye.
Dr. Khoramnia: I agree. In my experience, patients gain excellent visual acuity results across the entire range. Most patients achieve a visual acuity better than 20/20. That’s a huge plus right there, but also we aren’t spending time selecting anything in the OR, and we can focus directly on treating the patient.
Dr. Krueger: Sometimes, a patient won't qualify for a tomography-guided treatment, maybe because their maps are inconsistent or they have dry eye disease. Are there some patients who don’t qualify for treatment with the wavelight plus?
Dr. Bala: Performing a wavefront refraction and gathering other data can be challenging in eyes with a small pupil and individuals who accommodate a lot during measurement in dim lighting. Accounting for accommodation is important in treatment planning.
Dr. Krueger: Are there any tricks for that?
Dr. Bala: Keeping patients’ anxiety at bay can be helpful. We have a door open to let light into the room so that the patient is aware of their surroundings. We also tell them to look beyond the device’s target. If they are truly anxious at that moment, we take off the auto refraction and do a manual refraction instead. Worst case scenario, they can sit outside for a little while and come back in when they’re ready. Our failure rate dropped drastically after a short learning curve and staff buy-in. Some staff members can be resistant to any type of change because of historically excellent results, but in my practice they came around quickly. The duration of the testing became shorter, and the staff realized that this technology brings us closer to the goal of superior vision.
Dr. Krueger: For some surgeons, speed is imperative. Wavefront-optimized treatments are faster because they don’t require as much planning as tomography-guided treatments. But now that we can capture ray tracing with the wavelight plus, we can offer amazing customization and take visual outcomes to the next level.
Dr. Khoramnia: That’s why comparative studies are important. At the end of the day, a 2-minute time savings isn’t advantageous if you can’t provide maximal results.
Dr. Kanellopoulos: I think most patients would choose wavelight plus if they knew the advantages. We have the obligation to educate them on the technologies available.
MULTICENTER STUDY RESULTS
Dr. Krueger: Dr. Khoramnia, you were involved in a multicenter clinical study of the wavelight plus. Can you share your results?
Dr. Khoramnia: Dr. Bala, Dr. Kanellopoulos, and I participated in a post-market study looking at the wavelight plus treatment.12 For the study, patients had to be at least 21 years old with myopia as high as -11.00 D with or without astigmatism up to 4.50 D. All patients had a stable refraction and a corrected distance visual acuity of 0.04 logMAR or better before surgery. Patients with an ocular condition that may predispose the patient to complications, who underwent previous intraocular or corneal surgery, and those who were taking systemic drugs that could confound outcomes or increase the patients’ risk of complications were excluded from the study.
At 3 months, 212 eyes were available for follow-up. The absolute mean refractive spherical equivalent was 0.25 D or less, 0.50 D or less, 0.75 D or less, and 1.00 D or less in in 74.1%, 92%, 98.5%, and 99.5% of eyes, respectively (Figure 4).12 The visual acuity results are even more impressive—far better than I’ve ever seen with any other treatment modality. Most eyes (83.8%) achieved an uncorrected distance visual acuity (UDVA) of 20/20 or better by 1 week and 98.1% by 3 months postoperative.12 Almost 45% achieved 20/12.5 or better by 3 months.12 Additionally, about 95% of eyes achieved the same or better postoperative UDVA than their preoperative corrected distance visual acuity (CDVA) by 1 month postoperative. At 3 months, more than 26% gained at least 1 line of visual acuity (Figure 5). Additionally, about 36% of patients gained CDVA at 3 months, and only 0.5% lost CDVA (Figure 6).
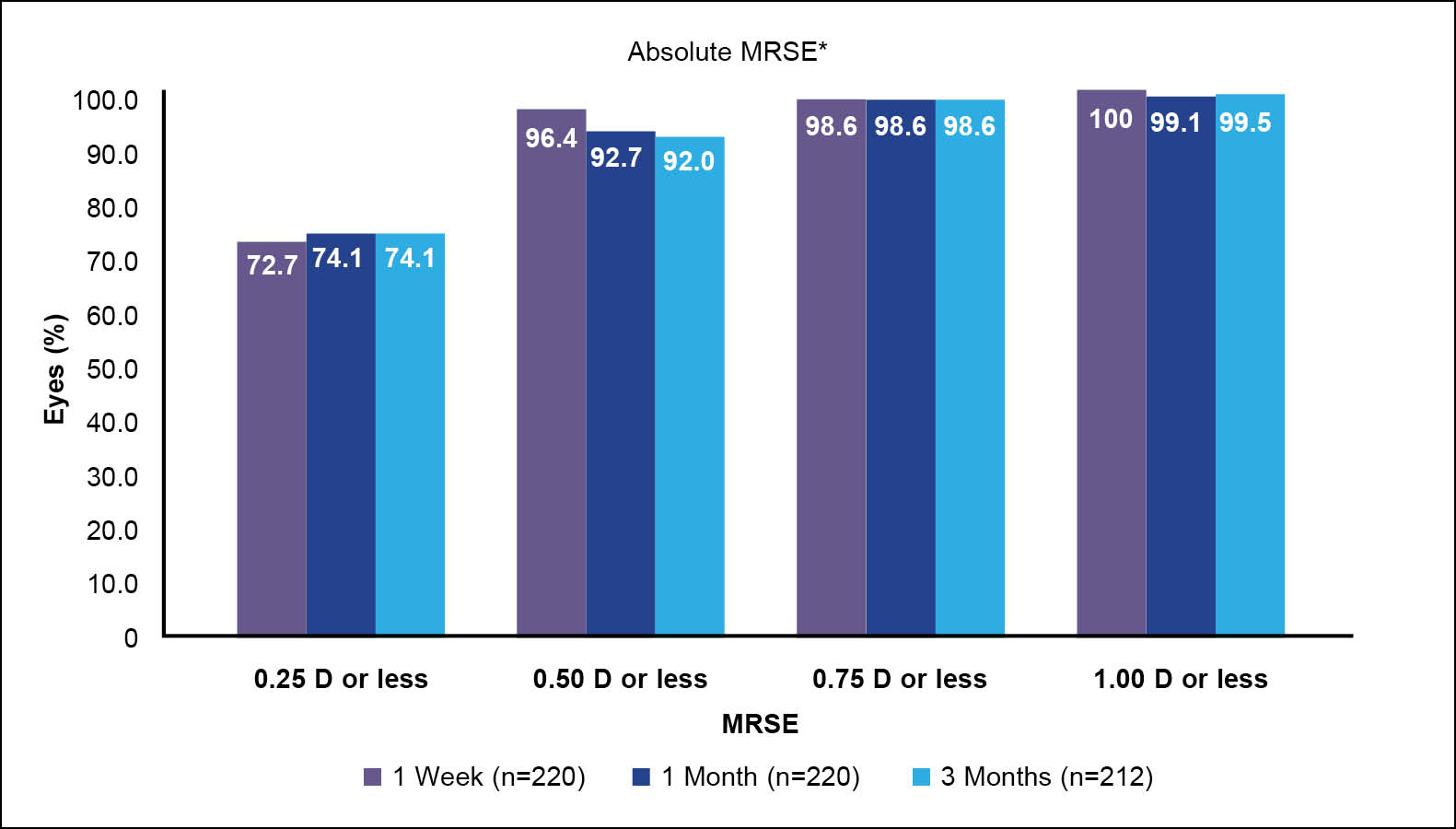
Figure 4. Mean refraction spherical equivalent at 3 months after treatment with wavelight plus in a multicenter clinical trial. 12
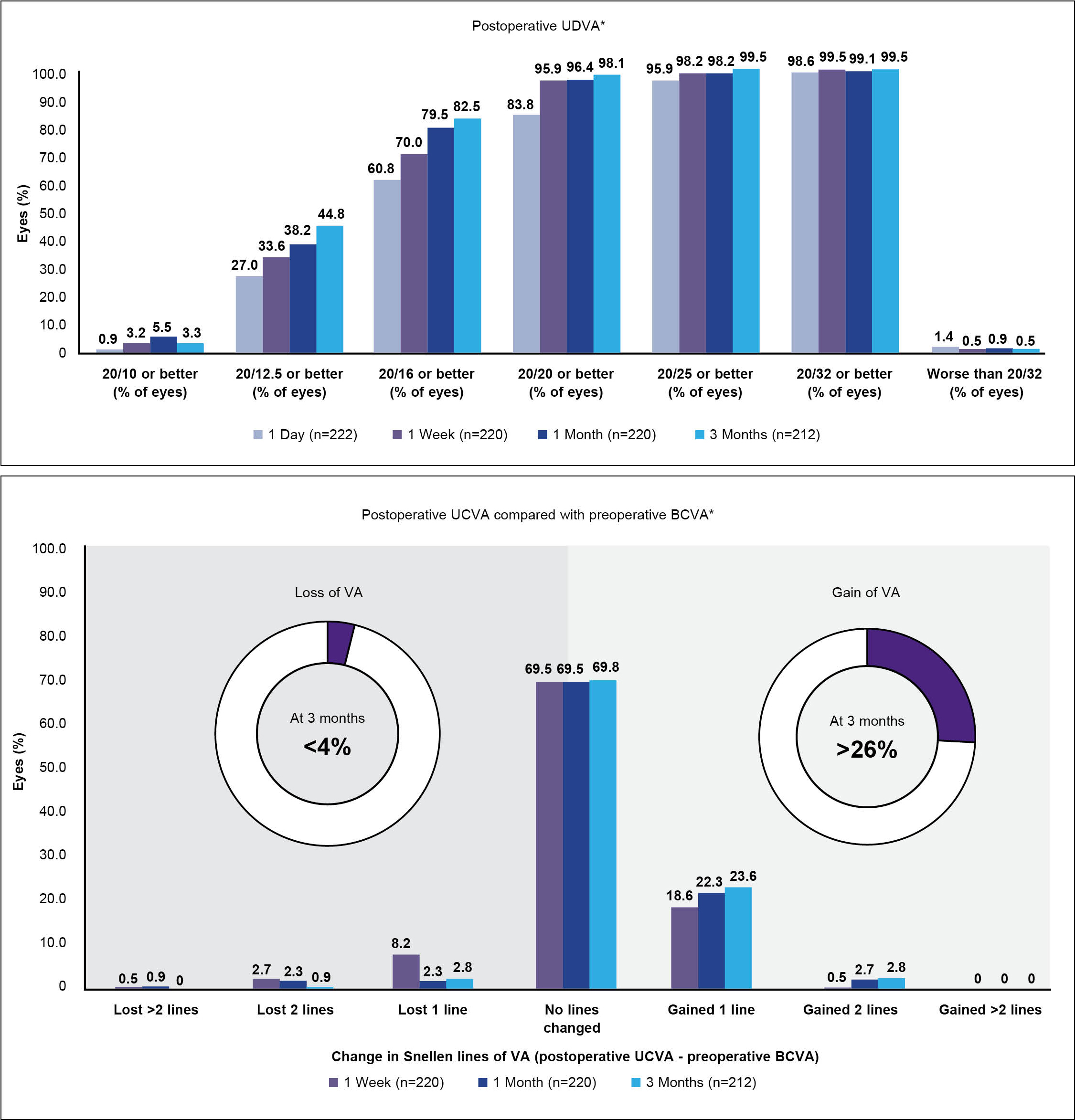
Figure 5. Visual acuity gains at 3 months after treatment with wavelight plus in a multicenter clinical trial.12
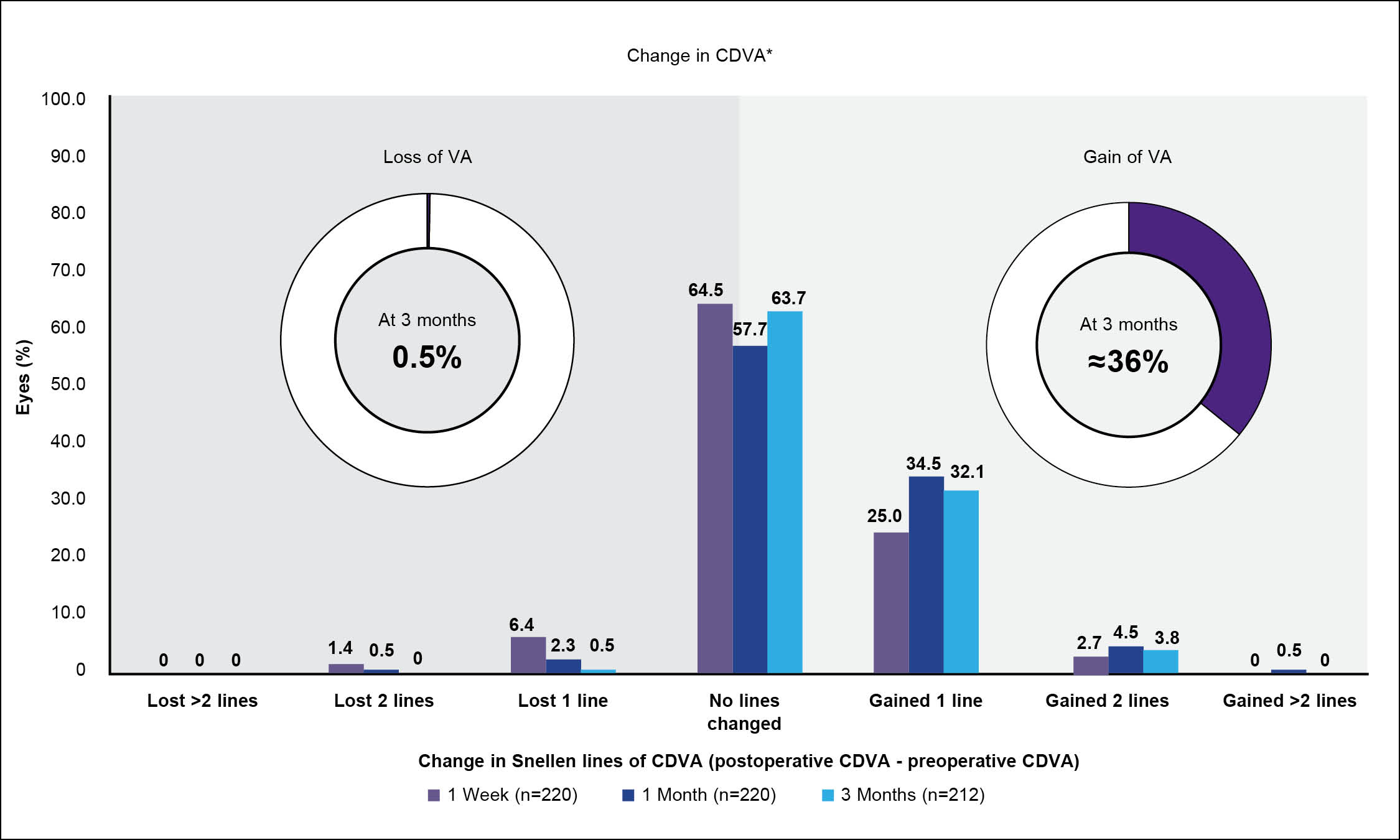
Figure 6. CDVA at 3 months after treatment with wavelight plus in a multicenter clinical trial.12
Patient satisfaction was high with the wavelight plus treatment. All patients fully or partially achieved their goals after surgery, and 99% said they would undergo the LASIK procedure again. Almost all (96.3%) were completely or very satisfied with their results. We concluded that wavelight plus clearly delivered predictable and reproducible clinical outcomes and provided better clinical results for the percentage of eyes achieving a CDVA of 20/20 or better compared to non-customized LASIK surgery.12,14
Dr. Krueger: I think we’re all impressed with the high numbers of patients who achieved not only 20/20, but also 20/16 and 20/12.5. There also was no significant increase in any of the HOAs in the study. So, we're correcting HOAs to improvement without the induction that normally is seen with any other correction.
Dr. Kanellopoulos: The beauty of this study is that predictable, reproducible, and consistent outcomes were achieved by different investigators in different clinical settings and not only in different countries but across different continents.
Dr. Krueger: When you can truly measure the aberrations, which is an objective number, and show no statistical worsening, then we know we’ve started to achieve the level of superior vision that we've been looking for.
Dr. Khoramnia: As clinicians, we appreciate understanding why we are getting good and consistent results with wavelight plus, but at the end of the day, the most important thing is that patients get excellent results.
PERSONAL EXPERIENCE
Dr. Krueger: How do the results of the multicenter clinical trial compare to the personal experience you have with wavelight plus in your clinic, Dr. Khoramnia? What is the selling point for patients about wavelight plus?
Dr. Khoramnia: In terms of planning, tomography-guided LASIK has always been more complicated than wavefront-guided LASIK, but that step is now going away with wavelight plus. We see excellent visual acuity results across the range consistently. In terms of patient satisfaction, comparative clinical studies are needed to show that wavelight plus is superior to traditional LASIK treatments.
Dr. Krueger: I would tend to agree. Most of the time, patients are happy after any LASIK treatment, but if you can get a higher percentage of them to 20/15 or 20/12.5 by doing a wavelight plus treatment, why wouldn’t you use this technology? It’s always better to have a little extra vision than you anticipated.
Dr. Khoramnia: Every patient will opt for the better procedure.
Dr. Bala: In my clinic, the results have been astonishing. I published a retrospective chart review of 3-month data from 400 eyes of 200 consecutive patients undergoing wavelight plus femtosecond LASIK for myopia between February and December 2022.20 The Sightmap was used for treatment planning in all cases. Patients were at least 18 years of age and had no more than -8.25 D of myopia with or without astigmatism up to 4.25 D. All patients had a stable refraction for a minimum of 12 months and both wavefront and subjective sphere within 0.50 D.
At 3 months, 89.5% of patients achieved a UDVA of 20/16, about 50% achieved 20/12.5, and 8% achieved 20/10; all eyes achieved a UDVA of 20/20 or better (Figure 7).20 Just under 40% gained 1 or more lines of visual acuity compared to their preoperative BCVA, and about 98.5% were within 1 line (Figure 8). Also at 3 months, 96.3% were within ±0.50 D of the absolute manifest refraction spherical equivalent and 96% were within ±0.50 D of astigmatism (Figure 9). There was no clinically significant increase in HOAs, and spherical aberration decreased despite 21% of patients having more than -5.00 D of sphere preoperatively.
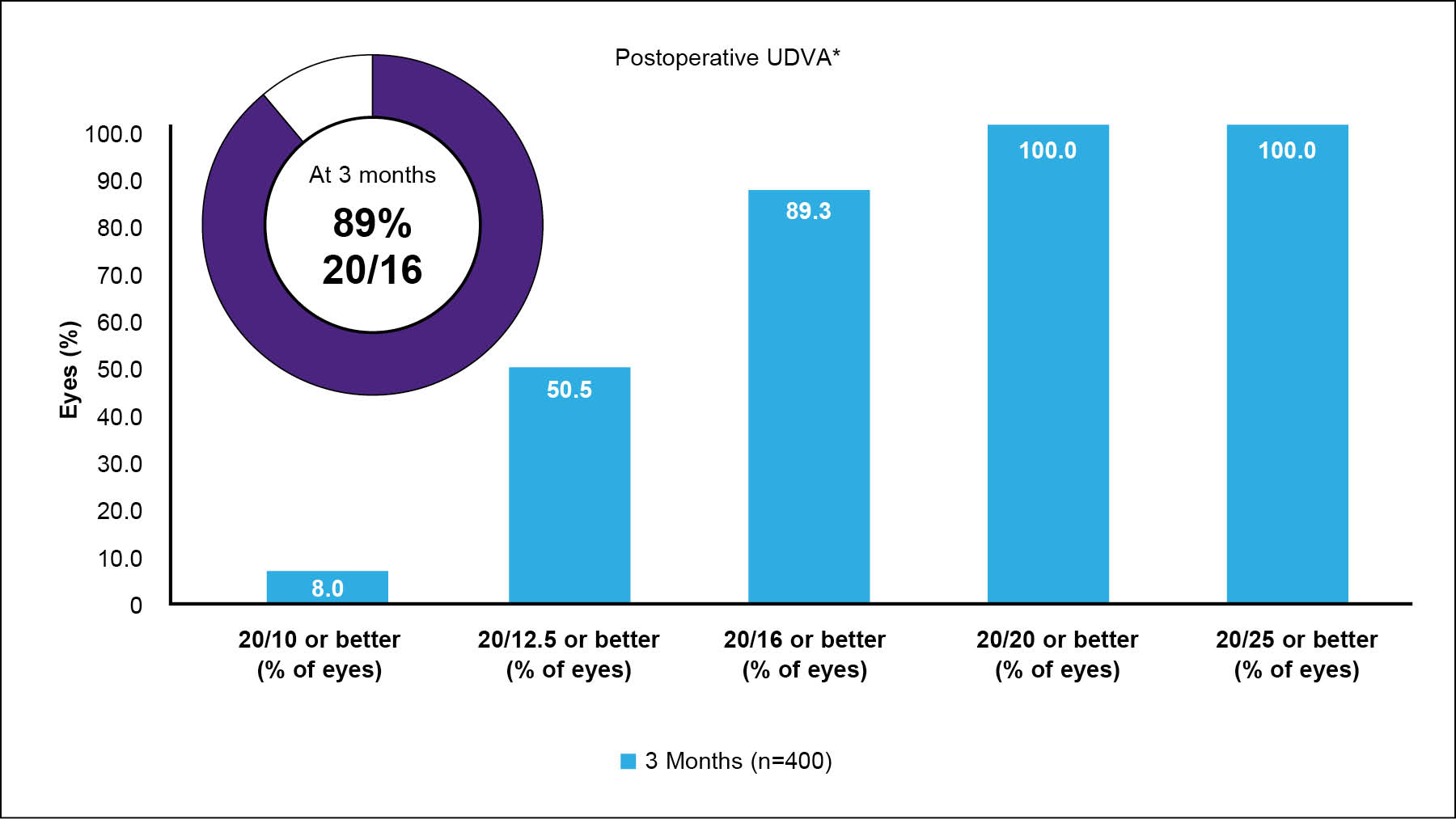
Figure 7. UDVA at 3 months after wavelight plus treatment at Dr. Bala’s clinic.20
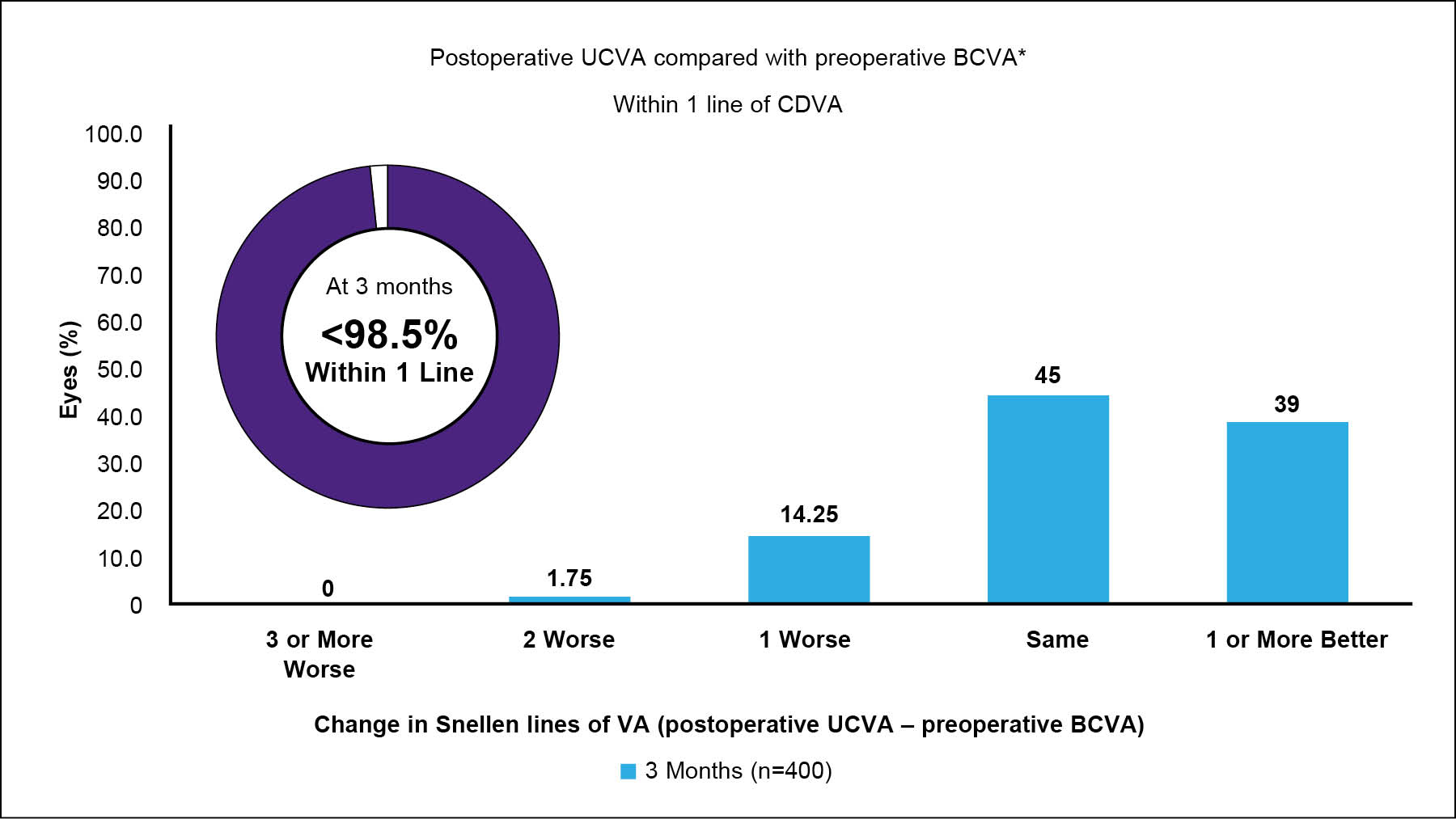
Figure 8. Visual acuity line gains at 3 months after wavelight plus treatment at Dr. Bala’s clinic.20
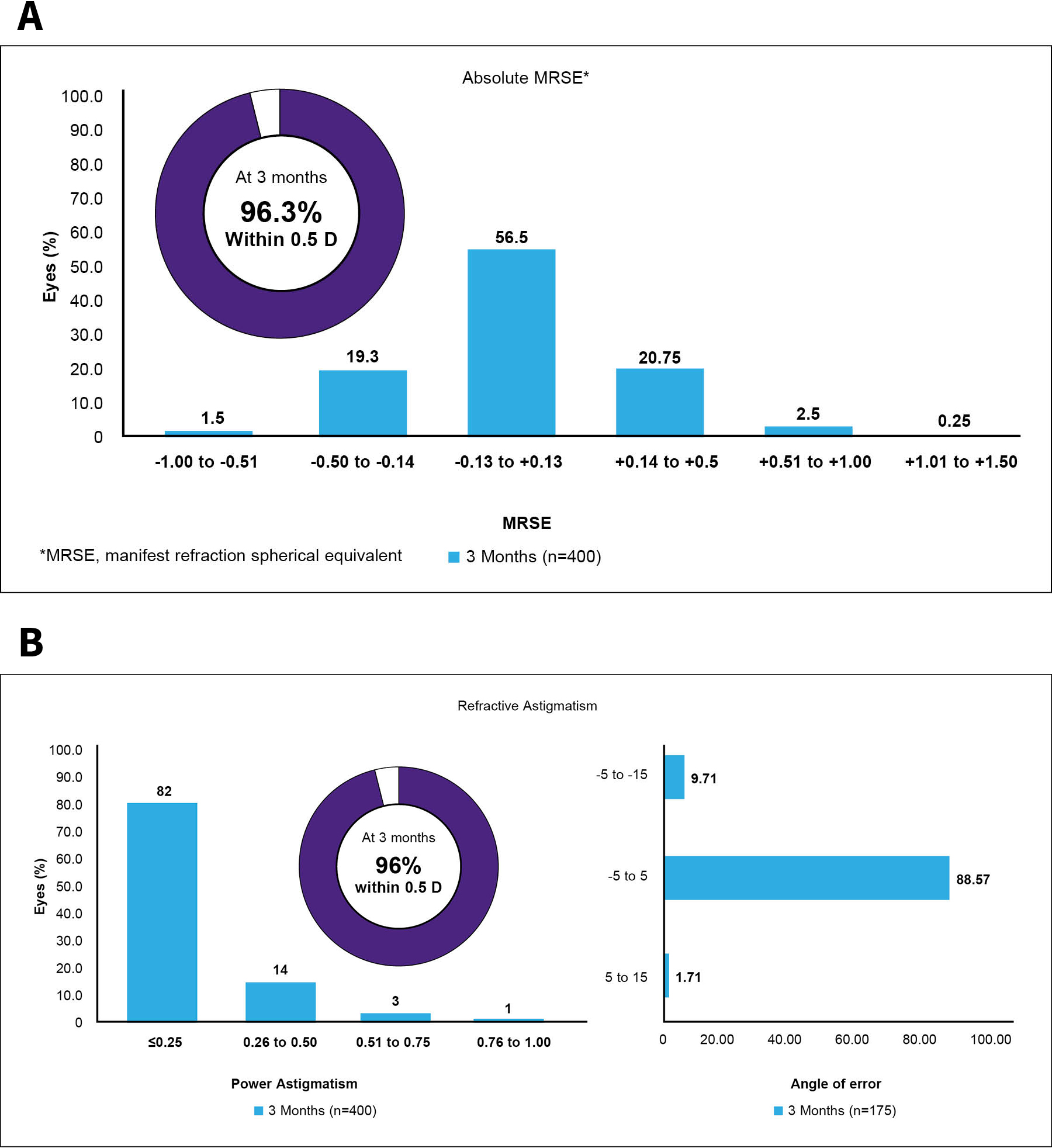
Figure 9. Absolute manifest refraction spherical equivalent (A) and astigmatism (B) at 3 months after wavelight plus treatment at Dr. Bala’s clinic.20
To me, the wavelight plus procedure holds great promise. I don’t have to spend as much time thinking about the treatment plan like I do with other treatments—it is basically done for me. I make sure that the refraction is accurate and the data collection process produces quality, unaccommodated measurements. Once I have done these things, the software does the rest. The outcomes speak for themselves.
Dr. Kanellopoulos: My personal experience mirrors Dr. Bala’s. Contoura Vision (Alcon), especially with the Tomography-Modified Refraction concept we introduced in 2014, opened the window for us to improve the lines of vision gain for patients. Now, wavelight plus can do this without all the previous lengthy and demanding work and calculations. We can also perform the procedure in a broader spectrum of patients, so it's a true win-win situation.
Dr. Krueger: This discussion has been extremely educational. I look forward to seeing how the wavelight plus technology rolls out on a worldwide level.
1. Barraquer J. History of refractive surgery. Highlights Ophthalmol. 1985;13(1):6-14.
2. Fyodorov SN, Durnev VV. Radial keratotomy for myopia. Vestn Oftalmol. 1978;94(6):37-41.
3. McDonald MB, Kaufman HE, Durrie DS, Rhee DJ. New perspectives on the correction of myopia: implications of the human genome for the development of laser refractive surgery. Arch Ophthalmol. 2002;120(6):871-878.
4. Pallikaris IG, Papatzanaki ME, Stathi EZ, Frenschock O, Georgiadis A. Laser in situ keratomileusis. Lasers Surg Med. 1990;10(5):463-468.
5. Ang M, Gatinel D, Reinstein DZ, et al. Refractive surgery beyond 2020. Eye. 2021;35:362-382.
6. Reinstein DZ, Carp GI, Archer TJ, Gobbe M. LASIK for myopia and hyperopia. Clin Ophthalmol. 2011;5:1045-1056.
7. Joffe SN. The 25th Anniversary of Laser Vision Correction in the United States. U.S. National Library of Medicine. 2021.
8. Lasik Eye Surgery Market. DataM Intelligence. 2021.
9. InnovEyes™ Sightmap Diagnostic DeviceUser Manual 1089
10. Mrochen M, Bueeler M, Donitzky C, Seiler T. Optical ray tracing for the calculation of optimized corneal ablation profiles in refractive treatment planning. J Refract Surg 2008;24:S446-445.
11. Schumacher S, Seiler T, Cummings A, Maus M, Mrochen M. Optical ray tracing–guided laser in situ keratomileusis for moderate to high myopic astigmatism. J Cataract Refract Surg. 2012;38:28-34.
12. Alcon data on file, 2021.
13. Kanellopoulos J, Maus M, Bala C, Hamilton C, Lemonis S, Jockovich ME, Khoramnia R. A88. International multicenter, prospective, myopic femtosecond-laser assisted myopic LASIK, customized by automated ray-tracing calculation of low and high order aberrations: a post-market study. 56th Panhellenic Ophthalmologic Congress (Hellenic Ophthalmological Society); June 8-10, 2023; Ioannina, Greece.
14. Cummings AB, Kelly GE. Optical myopic laser in situ keratomileusis: 1-year clinical outcomes. Clin Ophthalmol. 2013;7:1181-1191.
15. Dupps, W. Biomechanics and why surface ablation is so important. Paper presented at: the 5th International Congress on Epi-LASIK and LASEK Advanced Surface Ablation; September 8, 2006; London.
16. Huang D, Tang M, Shekhar R. Mathematical model of corneal surface smoothing after laser refractive surgery. Am J Ophthalmol. 2003 Mar;135(3):267-278. doi: 10.1016/s0002-9394(02)01942-6.
17. Kanellopoulos AJ, Asimellis G. In vivo three-dimensional corneal epithelium imaging in normal eyes by anterior-segment optical coherence tomography: a clinical reference study. Cornea. 2013;32(11):1493-1498.
18. Kanellopoulos AJ. Comparison of corneal epithelial remodeling over 2 years in LASIK versus SMILE: a contralateral eye study. Cornea. 2019;38(3):290-296.
19. Durrie D, Stulting RD, Potvin R, Petznick A. More eyes with 20/10 distance visual acuity at 12 months versus 3 months in a tomography-guided excimer laser trial: possible contributing factors. J Cataract Refract Surg. 2019;45(5): 595-600.
20. He G, Bala C. Ray-tracing–guided myopic LASIK: real-world clinical outcomes. J Cataract Refract Surg. 2023;49:1140-1146.
*wavelight plus is also known as InnovEyes.
Alcon medical devices comply with the current legislation for Medical Devices. Exclusive use by healthcare professionals. Please refer to relevant products DFU or Operator’s manuals for complete list of indications, contraindications and warnings.
© 2024 Alcon Inc. 1/24 JOB #




