
I am a cataract and refractive surgeon in Salt Lake City, Utah. In my 15 years of practice, I have participated in numerous clinical and FDA trials, including the FDA study for the EVO ICL (STAAR Surgical). Given the prevalence of high myopia in my region, the ICL has become a substantial component of my refractive surgical volume because it delivers excellent outcomes with high patient satisfaction.
Yet, this lens' preoperative workup is admittedly more demanding compared to procedures such as LASIK, and its accuracy has significant downstream consequences. In my opinion, this challenge has been the primary factor limiting broader adoption of the technology. Here, I will describe how a combination of technologies from Lumibird Medical—the ABSolu® ultrasound platform with linear UBM 50-MHz probe and the AI-powered ICLguru software from REVAI for calculating the size and power of ICLs—have made ICL calculations much more efficient and reliable in my clinic.
The Challenge of ICL Sizing
The technical aspects of ICL implantation are not complex, and its surgical placement is relatively straightforward. The real challenge lies in the preoperative decision-making, specifically the selection of the correct lens size. That decision is critical, and it must be made in an anatomic region of the eye that has historically been difficult to measure accurately and consistently.
Early ICL sizing strategies were based on white-to-white measurements. Even today, the FDA-approved sizing calculator relies on white-to-white. The limitation of this approach is well recognized: white-to-white is not a standardized measurement. Surgeons may obtain it manually, with optical biometry, or with tomography, and each method introduces variability. As a result, surgeons may arrive at different sizing decisions for the same eye that can lead to postoperative “surprises.” For surgeons early in their experience with ICLs, even one such outcome can be discouraging and deter continued adoption.
Moving Toward Sulcus-to-Sulcus Measurements
A logical evolution in ICL planning has been to image and measure the anatomy where the lens actually resides. Early in my career, ultrasound biomicroscopy (UBM) was already being used to visualize the anterior segment, and over time surgeons began incorporating sulcus-to-sulcus (STS) measurements into their sizing strategies. Surgeon-developed nomograms emerged, informed by correlations between STS measurements and postoperative outcomes.
While these approaches represented meaningful progress, they still depended on the ability to acquire high-quality images and to manually interpret and measure them. In practice, this process was highly operator-dependent and potentially time-consuming, particularly in high-volume settings.
Incremental improvements in diagnostic precision have always translated into more reliable surgical planning. Cataract surgeons have seen this repeatedly with advances in axial length measurement and keratometry. I view high-quality STS imaging as the analogous requirement for reliable ICL sizing.
The ABSolu® Ultrasound Platform
Having tried multiple competitive systems over the years, I find the quality of the images produced by the ABSolu® ultrasound platform to be superior. I attribute this image quality in large part to the system's linear 50-MHz UBM probe (Figure 1), which is designed to maintain consistent perpendicular alignment to anterior segment structures. From a practical standpoint, the probe's high resolution improves the definition of the sulcus and iridociliary anatomy, which are critical for STS assessment (Figure 2). With such a clear view of the relevant anterior segment structures, I have high confidence in its anatomic interpretation.
My team and I have used the ABSolu® for a little over 1 year. One of its most practical advantages is the automated STS measurement workflow, in which the software provides STS values directly without requiring me to manually place calipers on each image. As one should do with any automated system, I spent several months validating its landmark selection against those I would choose manually before I began relying on it routinely.
AI-Enhanced ICL Sizing and Vault Prediction
Even with high-quality STS data, the surgeon must still determine which ICL size is most appropriate. Historically, this decision relied on individual experience and limited datasets. Each practice's outcomes represented only a small fraction of the total available information.

Figure 1. The linear 50-MHz UBM probe on the ABSolu® ultrasound system is designed to stay perpendicularly aligned as it reveals anatomical structures in high-resolution detail.
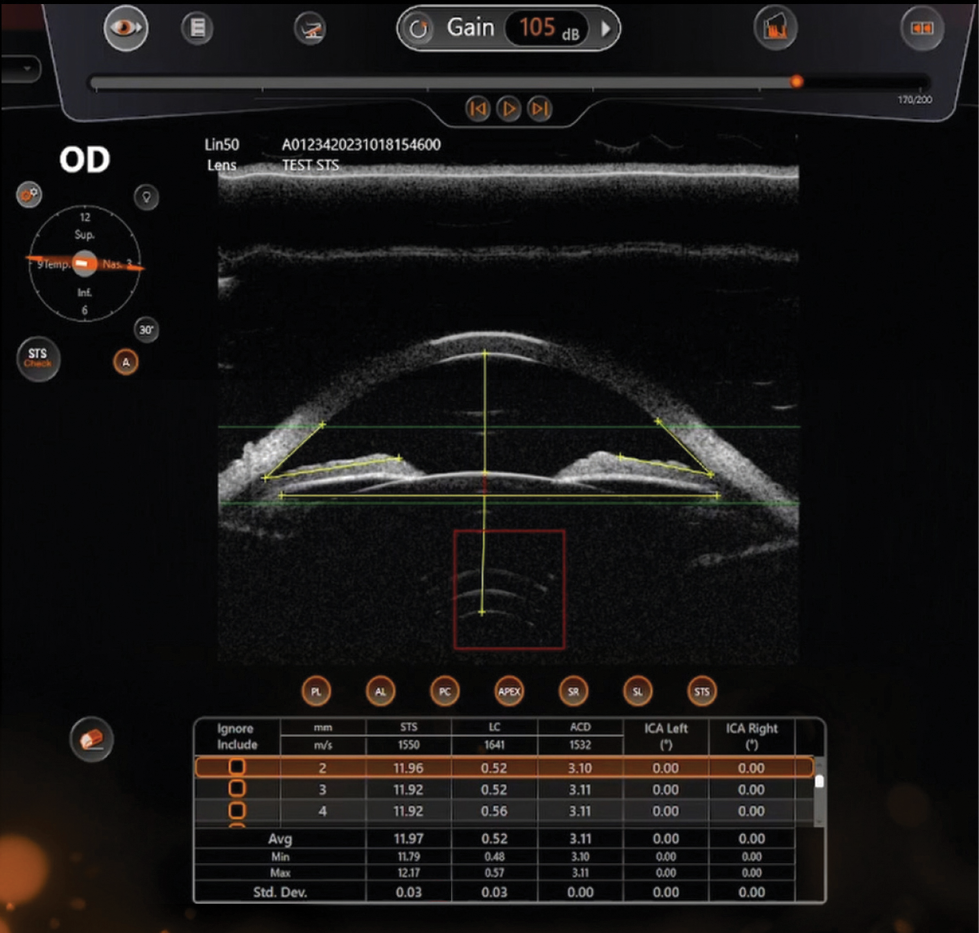
Figure 2. In the ABSolu's software, surgeons may review each line of the STS measurements.
This is where I believe ICLguru provides a significant additional benefit. By incorporating large datasets of images and clinical outcomes, the system generates two clinically actionable outputs: a recommended ICL size and a predicted postoperative vault (Figure 3). Importantly, it does not simply provide a recommendation; it also presents predicted vault values for each available lens size. This additional context is extremely valuable, particularly in borderline cases.
Conceptually, this capability represents a shift toward the efficiency cataract surgeons are accustomed to when selecting an IOL. While no predictive system is perfect, having a quantitative estimate allows for faster and more confident decision-making. In my experience, this has meaningfully reduced uncertainty in ICL sizing in my clinic.
A Streamlined, Technician-Driven Workflow
The workflow between the ABSolu© platform and the ICLguru is highly efficient, and it has significantly streamlined the workflow in my practice. Our technicians acquire all preoperative imaging in about 5 minutes. The imaging data, captured as a short video clip, transmits directly with the GURU Export from the ultrasound unit to the ICLguru (via Digital Imaging and Communications in Medicine [DICOM] connectivity). Within seconds, the ICLguru returns two key pieces of information: an STS image with an averaged measurement that I can visually confirm, and a single-page ICLguru report listing the four available ICL sizes, their predicted vaults, and a recommended size.
At my desk, I review the STS image with its averaged measurement and confirm that the bracket placement is anatomically appropriate. In tandem, I use the STAAR ICL calculator to select the lens' spherical and cylindrical power. With these tools, sizing selection takes me about 1 minute.
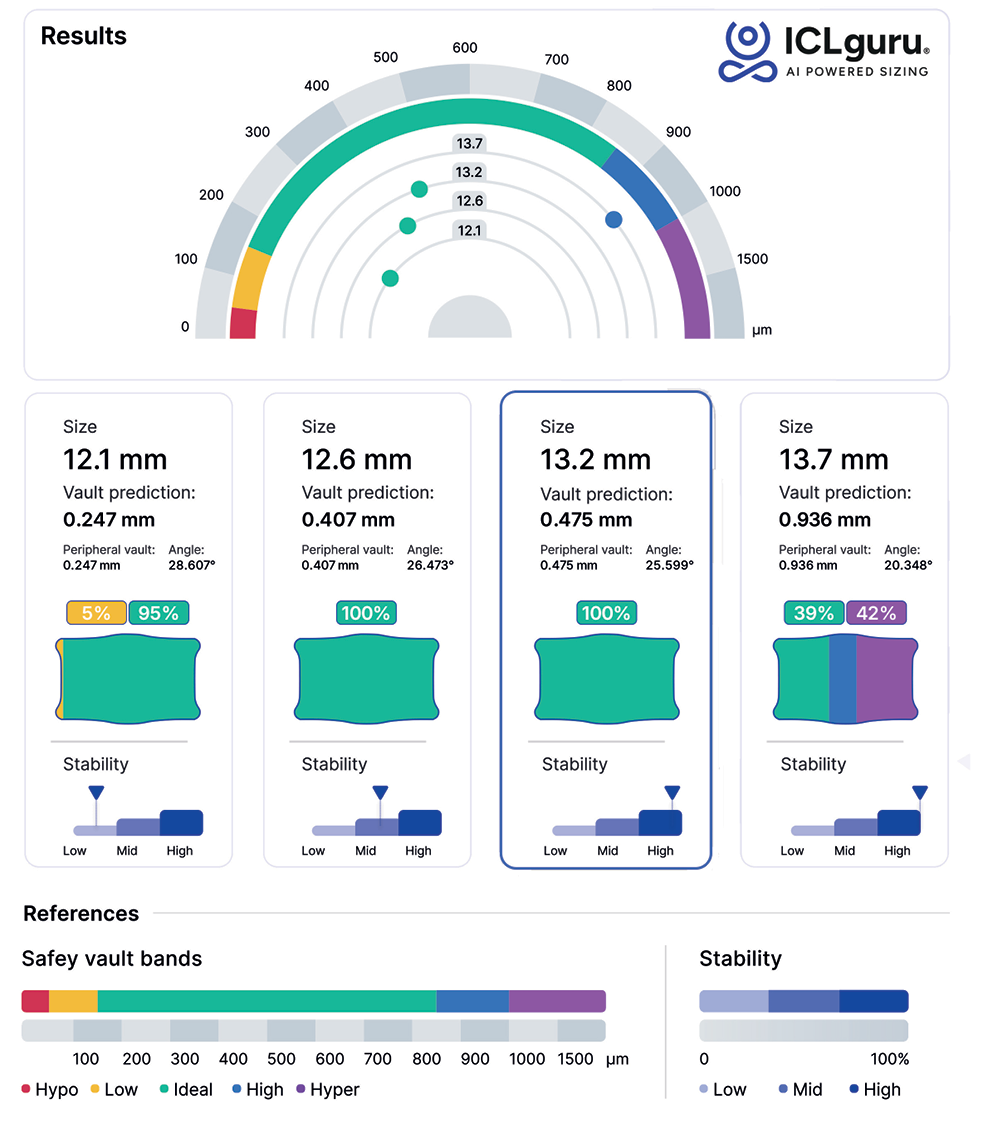
Figure 3. ICL calculations provided by the ICLguru software REVAI.
Removing Barriers to ICL Adoption
By combining high-quality UBM imaging, automated STS measurements, and AI-based size and vault prediction, the ABSolu® + ICLguru workflow addresses what has historically been the most significant limitation of the ICL procedure.
My team and I are actively collecting data comparing predicted vault values from the ICLguru with postoperative measurements, with the intention of eventually publishing these findings. While I do not yet have a formal dataset to share, anecdotally, the agreement between my predicted and observed postoperative vault has been strong. Over the past year, I can recall only one case that I would classify as a sizing surprise.
As these diagnostic and decision-support tools continue to mature, I expect they will enable both refractive and cataract surgeons to incorporate ICL surgery into their practices with greater confidence and consistency.
Disclaimer: Quantel Medical, by Lumibird Medical, is only ICLguru compatible, and the goal is only to send files to REVAI platform for ICL calculation. The images sent to REVAI platform have to be checked and validated by the user before sending.
Quantel Medical, by Lumibird Medical, cannot decide of the correct images sent to REVAI platform for ICL calculation. Quantel Medical, by Lumibird Medical, cannot be held responsible in case of ICL miscalculation

