
By combining the precision of a femtosecond laser and micron-accurate imaging, ViaLase has developed a noninvasive approach to reducing intraocular pressure (IOP) with a novel procedure called femtosecond laser, image-guided, high-precision trabeculotomy (FLIGHT). At a symposium held during the 2024 European Glaucoma Society Congress, a panel of experts discussed this new technology, as well as results from the first in-human study and the system’s potential to disrupt the conventional glaucoma treatment algorithm.
The Rise of Interventional Glaucoma
Elena Arrondo, MD: The conventional glaucoma treatment algorithm usually starts with prescribed topical medications followed by selective laser trabeculoplasty (SLT), microinvasive glaucoma surgery (MIGS), and filtration surgery. While these therapies can be effective, they each have some limitations.
We all know what happens when we prescribe topical medications for our glaucoma patients. Many patients don’t use the medications as prescribed, and 50% of patients stop using their drops just six months after starting treatment, which are behaviors that lead to disease progression.1 There are numerous risk factors for noncompliance with topical medications, including patient health beliefs and physical limitations; unpleasant side effects; complexity of the treatment regimen; and the cost of medications.2
Recently, we have seen a trend toward using SLT for initial therapy, particularly for patients who have ocular hypertension or mild glaucoma. In some patients, however, SLT is ineffective. As many as one-third of patients will not experience an IOP-lowering effect, and up to 60% of them will need retreatment.3
While MIGS procedures have relatively good safety profiles, they are, by definition, invasive. We must open the eye to perform MIGS, and we must use a hand-held gonioprism for visualization during the procedure, which can be difficult. In addition, patients prefer to avoid surgery, as noted by the lack of MIGS procedures performed outside of cataract surgery.
For many of our patients, particularly those with moderate or advanced glaucoma, filtration surgery may be the best treatment option. These surgeries are usually reserved as a last resort, as they are highly invasive and complicated, with a failure rate approaching 50% at 5 years.4 Given the various treatment options, we must decide which patients are the best candidates for filtration surgeries and which patients may not need such aggressive surgeries.
The new mindset in glaucoma practice is interventional glaucoma. This means intervening early in the disease process, avoiding topical medications with the accompanying risks for nonadherence and associated disease progression, and reserving the more invasive surgeries to treat advanced disease.5 By adopting this mindset, we also improve the patient’s experience, particularly when we employ a laser that will cause minimal disruptions in a patient’s life with immediate resumption of their daily activities. The ViaLuxe Laser System enables us to offer such a safe and effective incision-free procedure to lower IOP.
Glaucoma-Specific Technology
Marta Ibarz, MD, PhD: The ViaLuxe Laser System is a proprietary platform that combines the precision of a femtosecond laser with micron-accurate image guidance. It is designed to deliver tightly focused femtosecond laser pulses into the trabecular meshwork in a noninvasive way, creating precise channels in the angle with the goal of reducing IOP.
The chassis of the ViaLuxe system incorporates the femtosecond laser, OCT, gonio camera, manual docking delivery arm and head, and touch screen control system (Figure 1). The ViaVue™ handheld, high-definition gonio camera provides a 360° view of the trabecular meshwork, precluding the need for a gonioprism. This enables the surgeon to determine the best location for treatment in the iridocorneal angle without applying suction to the eye. The ViaLens™ is a proprietary, single-use patient interface with optical functionality that couples the patient to the laser. An innovative, curved design matches 99.6% of adult corneas and enables precise delivery of laser pulses into the trabecular meshwork while eliminating unwanted corneal distortions.
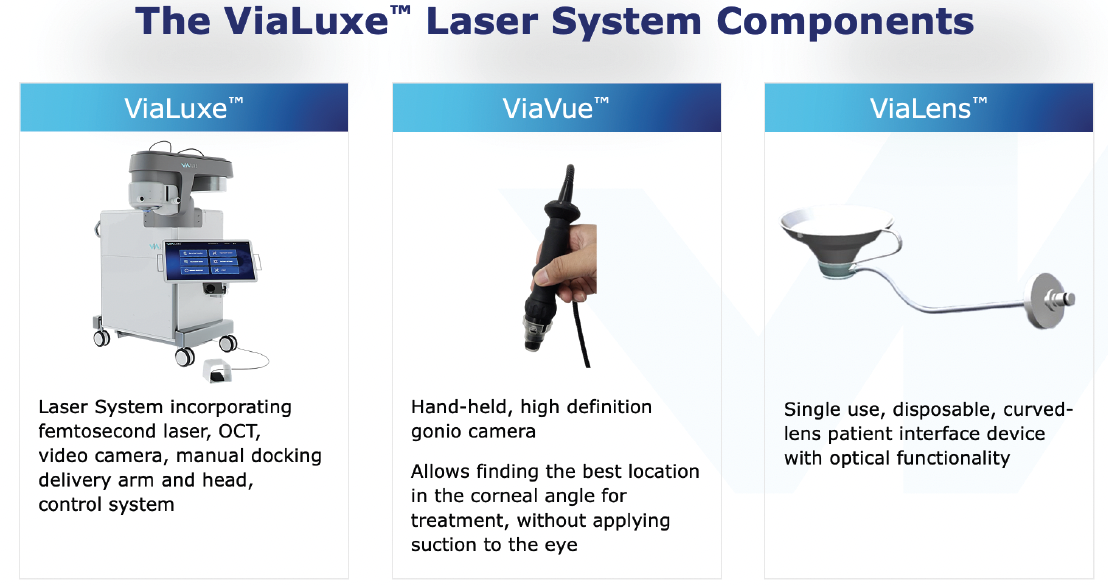
Figure 1. Each component of the ViaLuxe™ Laser System is designed to optimize a precise, noninvasive trabeculotomy.
This custom-engineered optimal scanning system delivers tightly focused pulses into the iridocorneal angle, thus creating micron-sized photodisruption sites within the target tissue without damage to adjacent tissues.
There are several key points of differentiation between the FLIGHT procedure and other angle-based interventions. They include:
1) The femtosecond laser creates a precisely defined aperture without opening the eye, thus mitigating the potential risks associated with incisional procedures.
2) A common and limiting requirement for some MIGS procedures is that they may be performed only during cataract surgery. By contrast, the FLIGHT procedure is performed as a completely incision-free standalone intervention.
3) The high-definition gonioscopic and micron-accurate OCT imaging overcomes traditional visualization limitations, and as we know, good visualization of the angle is directly associated with the probability of success in angle surgery (Figure 2).

Figure 2. The superior visualization provided by the ViaLuxe™ Laser System improves the potential for clinical success.
4) The ViaLuxe system gives surgeons access to all four quadrants of the trabecular meshwork, nasal and temporal areas alike. Right now, we are limited to treating the nasal quadrant, and we must use a hand-held gonioprism, which can change and distort the surgeon’s view and gives us little control over a patient’s movements. With the ViaLuxe system we can choose to treat any quadrant, and with the gonio camera, we avoid the difficulties we may encounter using a gonioprism.
Study: Excellent Safety Profile, Durable IOP Reduction
Andrew Tatham, MD: The first in-human study of the FLIGHT treatment was published in Ophthalmology Science in 2023.6 This study included 18 eyes of 12 patients who were monitored for two years at a single center in Budapest. About one-third of the patients had mild disease, one-third had moderate disease, and one-third had advanced disease. All of the patients underwent FLIGHT, during which the surgeon created a single 500 µm x 200 µm channel through the trabecular meshwork and into Schlemm’s canal.
In terms of safety, the results were quite encouraging. There were no serious adverse events related to the FLIGHT procedure. There were no cases of IOP spike, corneal edema, or hypotony, as might be expected with surgery targeting this pathway.
At baseline, mean IOP was 22.3 mmHg. At one week, mean IOP was 14.8 mmHg, and the reduction was sustained throughout the two years of the study. After a single treatment, IOP was still 14.5 mmHg at 24 months, which equates to a 34.6% reduction in mean pressure. In terms of absolute pressure reductions, almost 90% of eyes achieved pressures of 18 mmHg or lower, and 82% of eyes achieved more than a 20% pressure reduction (Figure 3). These results are encouraging in terms of safety, and they’re exciting in terms of efficacy.
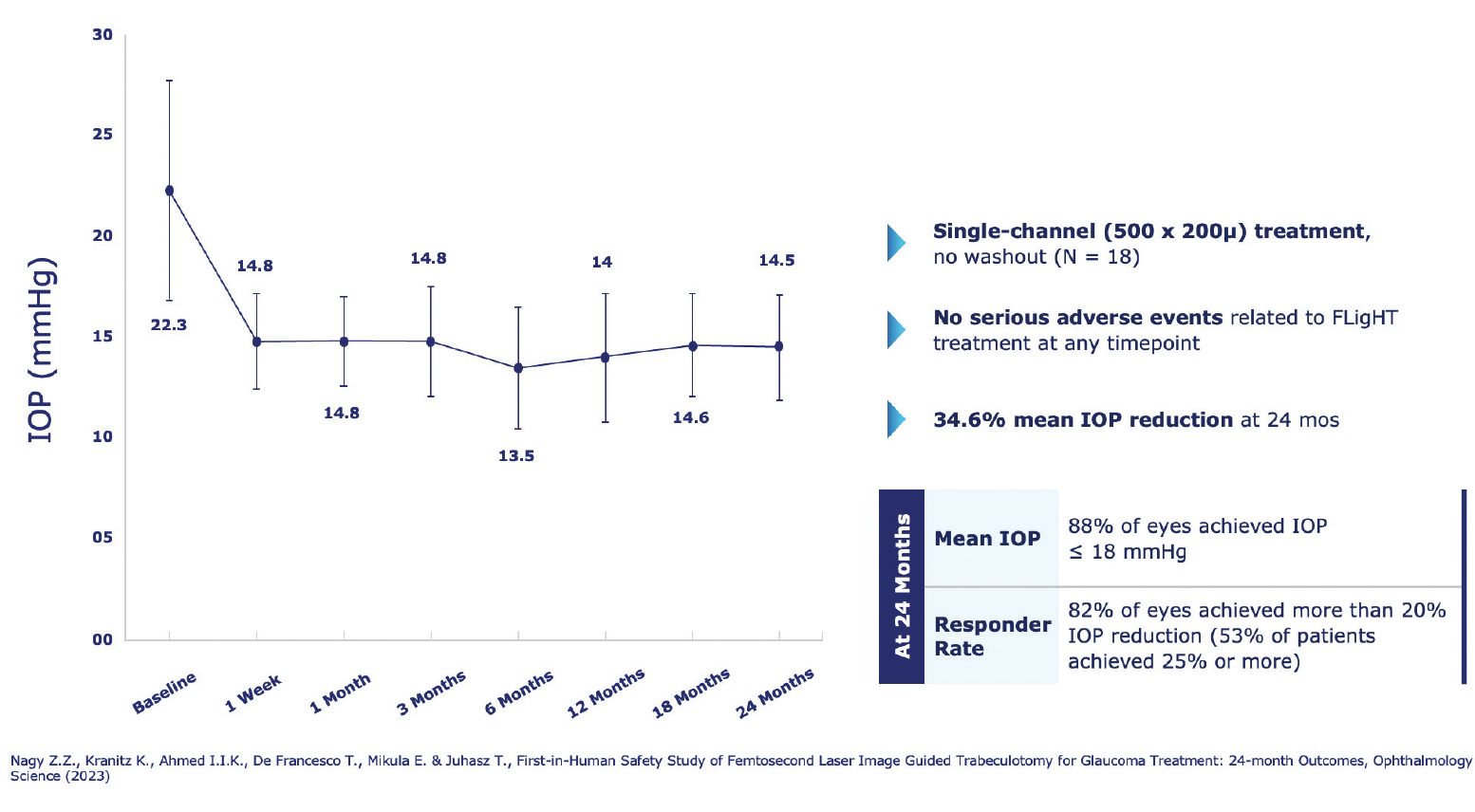
Figure 3. Investigators reported positive safety and efficacy results from the first in-human study of FLIGHT.
At two years, there was no evidence of aperture closure or scarring (Figure 4), which may explain the sustained reduction in IOP.

Figure 4. Channels created during FLIGHT remained patent at 24 months.
Some people might be concerned about collateral damage with this laser. The good thing about femtosecond lasers is that they’re cold lasers, so they do not cause thermal damage to the adjacent tissues. When we look at histology from eyes that were treated with FLIGHT, we can see that (Figure 5).
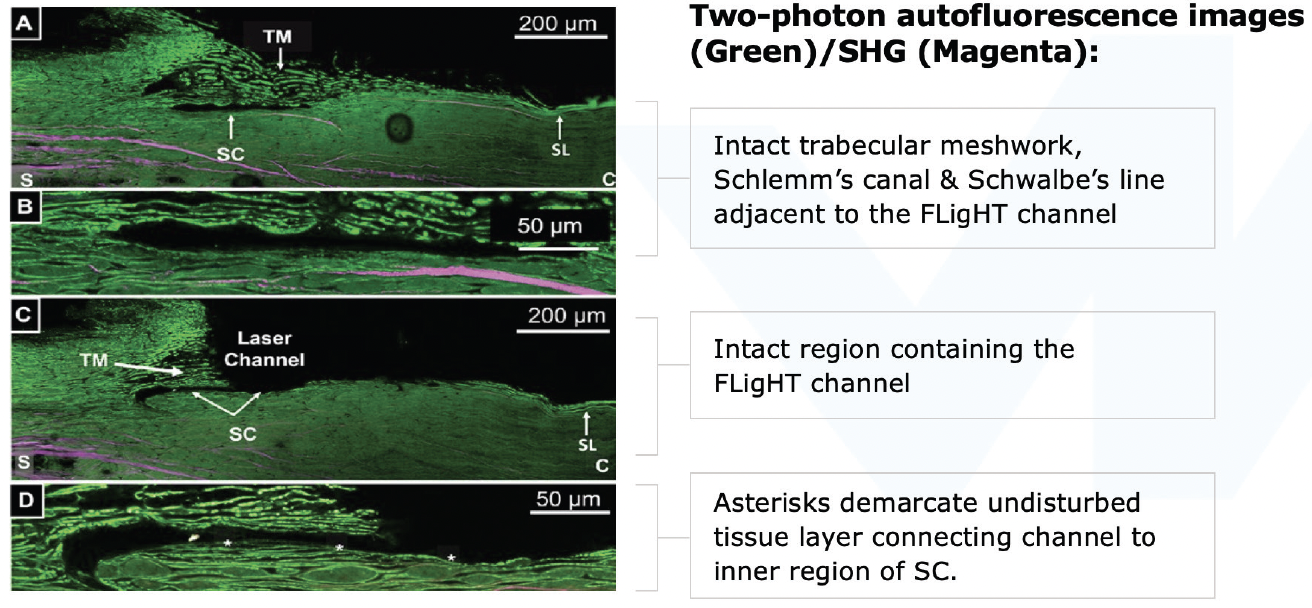
Figure 5. An advantage of using femtosecond lasers for this treatment is that they are cold lasers and do not cause thermal damage.7 Reprinted with permission from Translational Vision Science & Technology.
I believe the evidence thus far is extremely encouraging in terms of safety but also in terms of a fairly immediate IOP reduction, a lack of pressure spike, and a low need for postoperative steroids. Then there’s the sustained reduction in pressure, which is backed up by what we know about femtosecond lasers, and also from the histological and anterior segment OCT imaging. This is very exciting.
Candidates for FLIGHT
Karsten Klabe, MD: Good candidates for FLIGHT will have an open angle, a visible trabecular meshwork, and a clear cornea. Patients who have mild, moderate, or possibly severe glaucoma, whether stable or unstable, are all potential candidates. We also should consider FLIGHT for patients who struggle to adhere to or persist with a prescribed regimen of topical medications, whether their difficulties stem from adverse reactions, complexity of regimen, physical or mental limitations, or cost.
There are also procedural considerations when identifying candidates for a glaucoma surgery. Importantly, the pool of potential candidates for FLIGHT includes phakic and pseudophakic patients, as well as post-SLT patients and patients who previously underwent trabecular meshwork bypass surgery that failed.
When evaluating a new procedure for my patients, my first thought is about safety, not efficacy. Is the procedure safe, with no risk of infection, bleeding, or cataract formation? With safety in mind, would I consider a MIGS procedure for a patient who has had SLT? If it’s safe enough, yes, I would. How about for a phakic patient? I would not consider MIGS, which requires opening the eye, for such a patient. Because of the unique characteristics of the ViaLuxe Laser system, in my opinion, there is no limitation to offering FLIGHT to any of these patients.
I also believe it’s easier to perform FLIGHT at an early stage of glaucoma, and, with no risk of cataract formation, I would offer it very early to my phakic patients. In cases where a patient previously underwent glaucoma surgery in the nasal quadrant, FLIGHT is still an option because this laser enables us to treat all four quadrants of the iridocorneal angle.
Conclusion
Dr. Klabe: FLIGHT performed with the ViaLuxe Laser System is a new and unique incision-free procedure that we can safely offer to a broad spectrum of patients very early in the disease stage. This procedure gives us opportunities to treat both phakic and pseudophakic patients, even those who have had previous glaucoma surgeries.
FLIGHT has the potential to disrupt the current glaucoma treatment algorithm, even as the algorithm continues to evolve. As SLT is becoming our choice for initial therapy with topical drops playing an adjunctive role in some patients, FLIGHT may find its place as the next option in the algorithm, with the potential to address the largest patient segment compared to currently available treatments.
1. Quaranta L, Novella A, Tettamanti M, Pasina L, Weinreb RN, Nobili A. Adherence and Persistence to Medical Therapy in Glaucoma: An Overview. Ophthalmol Ther. 2023;12(5):2227-2240.
2. Moore SG, Richter G, Modjtahedi BS. Factors Affecting Glaucoma Medication Adherence and Interventions to Improve Adherence: A Narrative Review. Ophthalmol Ther. 2023;12(6):2863-2880.
3. Narayanaswamy A, Sood SR, Thakur S. Selective laser trabeculoplasty: An updated narrative review. Indian J Ophthalmol. 2024;72(3):312-319.
4. Gedde SJ, Feuer WJ, Lim KS, et al. Treatment Outcomes in the Primary Tube Versus Trabeculectomy Study after 5 Years of Follow-up. Ophthalmology. 2022;129(12):1344-1356.
5. Radcliffe NM, Shah M, Samuelson TW. Challenging the “Topical Medications-First” Approach to Glaucoma: A Treatment Paradigm in Evolution. Ophthalmol Ther. 2023;12(6):2823-2839.
6. Nagy ZZ, Kranitz K, Ahmed IK, De Francesco T, Mikula E, Juhasz T. First-in-Human Safety Study of Femtosecond Laser Image-Guided Trabeculotomy for Glaucoma Treatment: 24-month Outcomes. Ophthalmol Sci. 2023;3(4):100313.
7. Eric R. Mikula, Ferenc Raksi, Iqbal Ike Ahmed, Manu Sharma, Guy Holland, Reza Khazaeinezhad, Samantha Bradford, James V. Jester, Tibor Juhasz; Femtosecond Laser Trabeculotomy in Perfused Human Cadaver Anterior Segments: A Novel, Noninvasive Approach to Glaucoma Treatment. Trans. Vis. Sci. Tech. 2022.




