
Key Takeaways
- High predictability and consistency of postop results
- Excellent visual acuities at all ranges (distance, intermediate and near starting from 33 cm) improving from 1 to 3 months
- True continuous vision from distance through near (33 cm) without peaks or gaps, with near vision dramatically improved
- Great extended depth of focus of 4.5 D (plotted results) in the high-vision zone (between 0.20 and 0 logMAR) to deliver full presbyopia correction
- High-quality vision: Very good contrast sensitivity, comparable to a monofocal IOL, and within the normal values in all light conditions. No to very low incidence of photic phenomena
- Works well even in patients with some ocular pathologies, such as early macular degeneration, as tested by clinical use
- Very high patient satisfaction based on quality-of-life assessment
- Very high spectacle independence in different situations of everyday life and light conditions
- Faster neuroadaptation compared to diffractive multifocal IOLs
- The bilateral implant provided a natural functional vision close to the natural vision of the human eye
The WELL Fusion Optical System addresses all the unmet needs in presbyopia correction providing uninterrupted vision at all distances and in all light conditions, spectacle independence, improvements in near vision (vs standard EDOF IOL), negligible photic phenomena, and good contrast sensitivity.
Gerd U. Auffarth, MD, PhD, FEBO: Patient satisfaction is at the core of successful cataract surgery. According to results of a recent study published by CRST, the top three objective outcome goals that lead to high patient satisfaction with presbyopia-correcting IOLs are maximizing intermediate/near visual acuity, minimizing residual refractive error, and maximizing distance visual acuity and visual quality.1 Another thing that is important is spectacle independence, which, according to the 64% of surgeons included in the study, is the most important outcome to maximize patient satisfaction.1 On average, however, only 70% of patients who receive a presbyopia-correcting IOL are happy with their level of visual quality, and only 66% are happy with their level of dysphotopsia at 1 month postoperatively. Patient education and selection are therefore crucial to making sure patients are pleased with their outcomes and have the best chance at achieving excellent visual acuity and quality at all distances.
Patients want to have it all, but as we know there is always some kind of trade-off between vision quality, depth of field, and dysphotopsia. As the depth of field increases, so do dysphotopsias, and then visual quality decreases. The reason for this—especially with diffractive technology—is how depth of field and dysphotopsia are related to each other. Multifocal IOLs can partially satisfy patients’ expectations, but they also produce gaps in the range of vision and are associated with halos, glare, and reduced contrast sensitivity.2 Patients are usually not 100% happy with their intermediate vision, and many lenses, including trifocal IOLs, put the least amount of light energy in the intermediate focus. Usually, the distance focus gets the most light, followed by near and then intermediate. This does not work for all patients. Extended depth of focus (EDOF) IOLs, on the other hand, perform very well at intermediate and distance but not at near.2
The largest unmet need for patients today is therefore to provide a nondiffractive IOL design that guarantees good near vision and does not induce dysphotopsia. One novel solution, the WELL Fusion Optical System (SIFI), is poised to address all the unmet needs in IOL design, including increased spectacle independence, improvements in near vision, reduction in photic phenomena, and very good contrast sensitivity. The WELL Fusion Optical System achieves trifocality while avoiding the induction of dysphotopsia. It provides a full range of vision through both eyes. By balancing out the three focal areas—distance, intermediate, and near—you can reduce the dysphotopsia and still achieve a very good depth of field.
The WELL Fusion is a unique optical system that combines two EDOF IOLs: the Mini WELL IOL, which is well-established in the current marketplace, and the Mini WELL PROXA (both by SIFI), which is specifically designed to enhance near vision to deliver uninterrupted high-quality vision at all distances and in all lighting conditions (Figure 1).
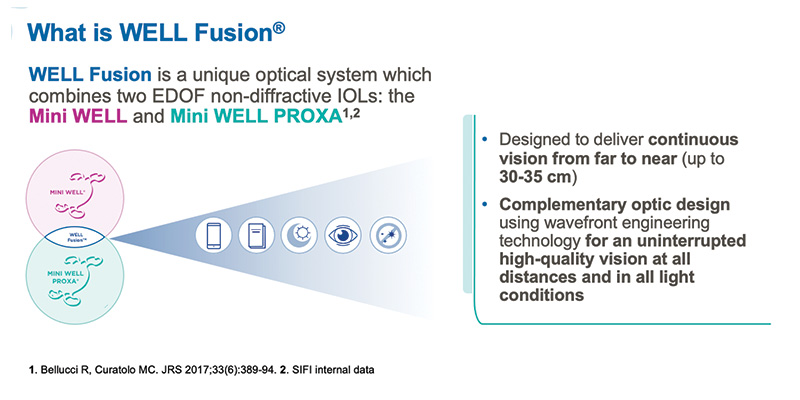
Figure 1. WELL Fusion is designed to deliver continuous vision from far to near (up to 30-35 cm).
The Mini WELL and Mini WELL PROXA IOLs have two complementary optic profiles and are identical in terms of biocompatibility, mechanical performance, and technical characteristics (Figure 2). They share the same EDOF, nondiffractive platform and are designed to induce targeted amounts of spherical aberration in concentric optical zones in the central part of the optics to extend depth of focus. The Mini WELL and Mini WELL PROXA are designed to be implanted together to jointly ensure continuous vision from distance to near (up to 30-35 cm), creating the WELL Fusion system. The Mini WELL PROXA lens incorporates a number of zones higher than the Mini WELL to extend the range of near vision.
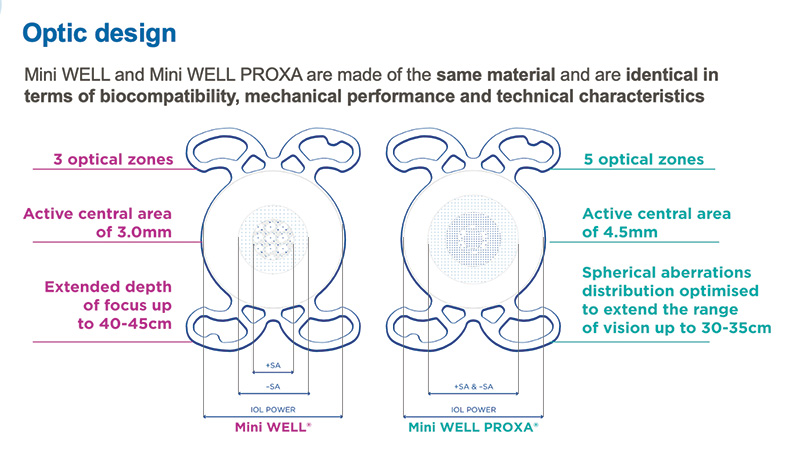
Figure 2. The Mini WELL and the Mini WELL PROXA IOLs share the same EDOF platform using targeted amounts of spherical aberration in the central part of the optics to extend the depth of focus.
Dr. Barraquer, please tell us more about the WELL Fusion System.
Elena Barraquer, MD: The combination of these two lens designs creates a binocular defocus curve without the peaks and valleys seen with trifocal IOLs. Additionally, the absence of visual gaps contributes to significantly reducing halos and glare and the complementary aberrometric pattern quick neural adaptation (Figure 3).3,4 (Editor’s note: For more on this topic, see Neural Adaptation With the WELL Fusion, by Leonardo Mastropasqua, MD). It increases the depth of focus and does so while avoiding the trade-off of dysphotopsias. Thus far in my experience, patient satisfaction with daily life activities is high with WELL Fusion. Patients report excellent spectacle independence at all distances with no need for reading glasses and very low light dependence. As a result, I find that the WELL Fusion system is a much better option than trifocal IOLs that are generally associated with a quality of vision that is not always as clear as we would like, require patients with a specific morphology of the eye (especially the cornea), and result in more complaints from patients that have a longer neuradaptation process and loss of contrast sensitivity especially in low light conditions.
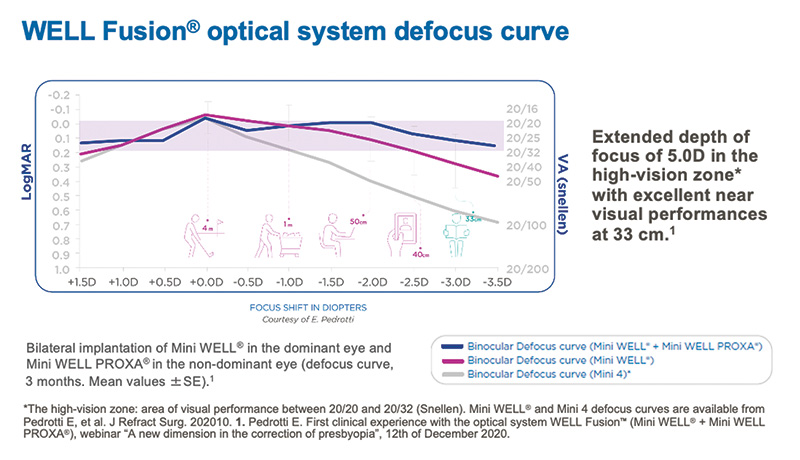
Figure 3. The WELL Fusion optical system defocus curve compared to the binocular defocus curves of the EDOF IOL Mini WELL and the monofocal IOL Mini 4.
PERSONAL EXPERIENCES
Based on global collective experiences with WELL Fusion, the system delivered excellent outcomes and high-quality vision across all distances from far to near up to 33 cm. Patients reported a very high level of spectacle independence in different situations of everyday life and in various lighting conditions.
Professor Auffarth: The goal of our discussion is to share our personal experience in regard to the WELL Fusion Optical System, including patient selection criteria and postoperative pearls. Before we talk about our personal experiences and data, I want to highlight the overall global data from our eight international sites, which includes 88 patients with a mean age of 62 years (total 166 eyes). The sites were the University Clinic Heidelberg in Germany, Centro de Oftalmología Barraquer in Spain, Eye & Vision Institute in the Philippines, University of Palermo in Italy, University Gabriele d’ Annunzio of Chieti in Italy, Oculens Eye Clinic in Romania, University of Verona in Italy, and Alpha Ophthalmological Center in Romania.
In all cases, the Mini WELL was implanted in the dominant eye and the Mini WELL PROXA in the nondominant eye with a target refraction of emmetropia. Follow-up examinations occurred on day 1 and week 1 and months 1 and 3. A total of 78 patients were available for follow-up at 3 months.
Overall results of these collective experiences are found in Figures 4 through 9. In short, patients experienced excellent postoperative outcomes, including an improvement in visual acuity from 1 to 3 months postoperative and achieved very good visual acuities at all distances, including near at both 40 and 33 cm. Additionally, patients expressed that they achieved true continuous vision from distance to near (33 cm) and achieved an extended depth of focus of 4.50 D, demonstrating a full presbyopia correction. Also, the flat defocus curve up to 33 cm really differentiates the WELL Fusion System from trifocal IOLs and has truly exceeded our expectations with near vision dramatically improved.
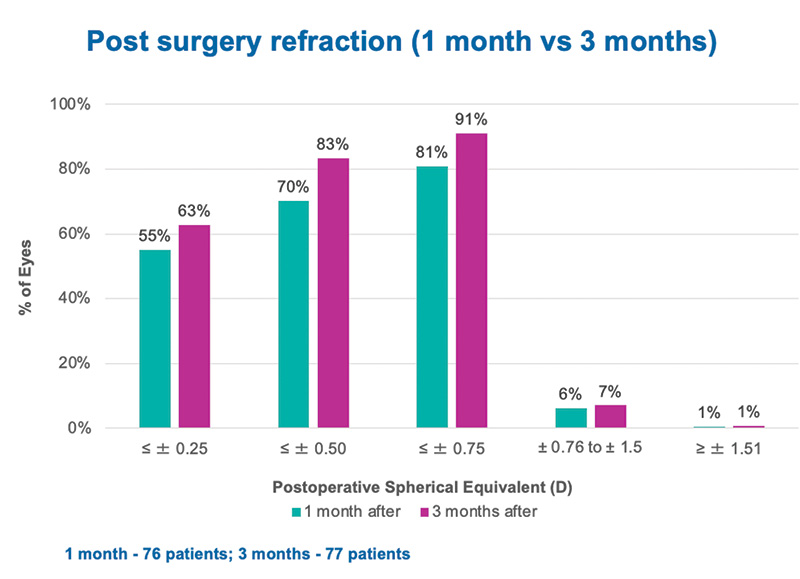
Figure 4. Post-surgery refraction showed improvement from 1 month to 3 months, as well as good predictability: 83% of patients achieved < 0.5 at 3 months.
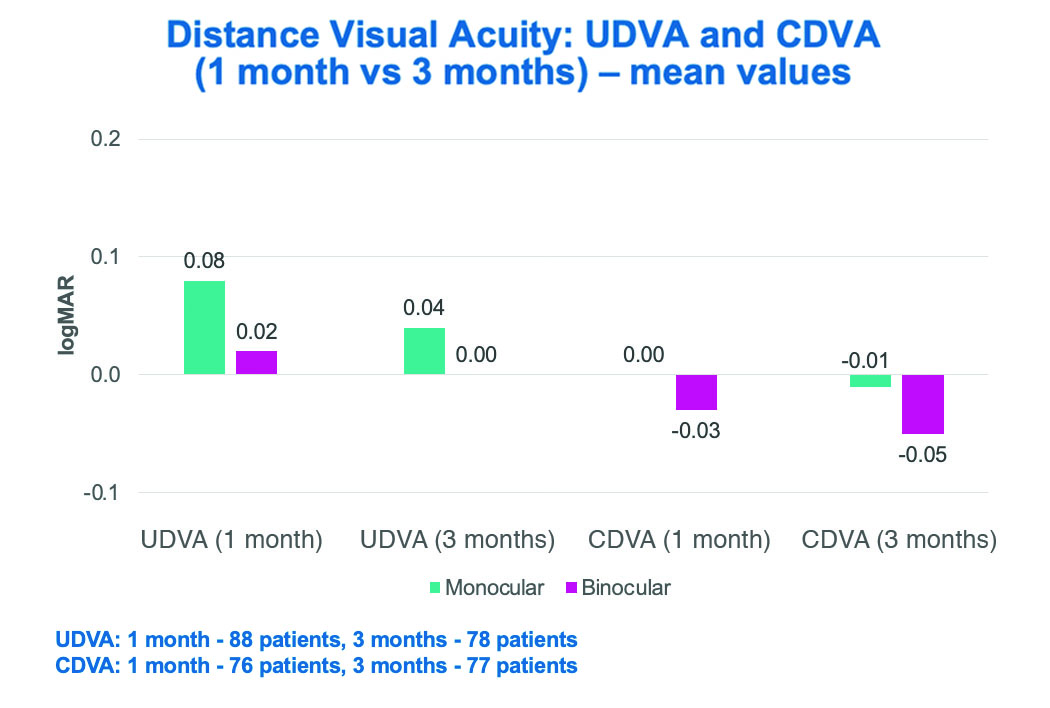
Figure 5. Mean values of uncorrected and corrected distance visual acuity at 1 and 3 months
postoperative. Both UDVA and CDVA were shown to improve over this time period, with excellent
CDVA demonstrated at 3 months.
UDVA: uncorrected distance visual acuity; CDVA: corrected distance visual acuity
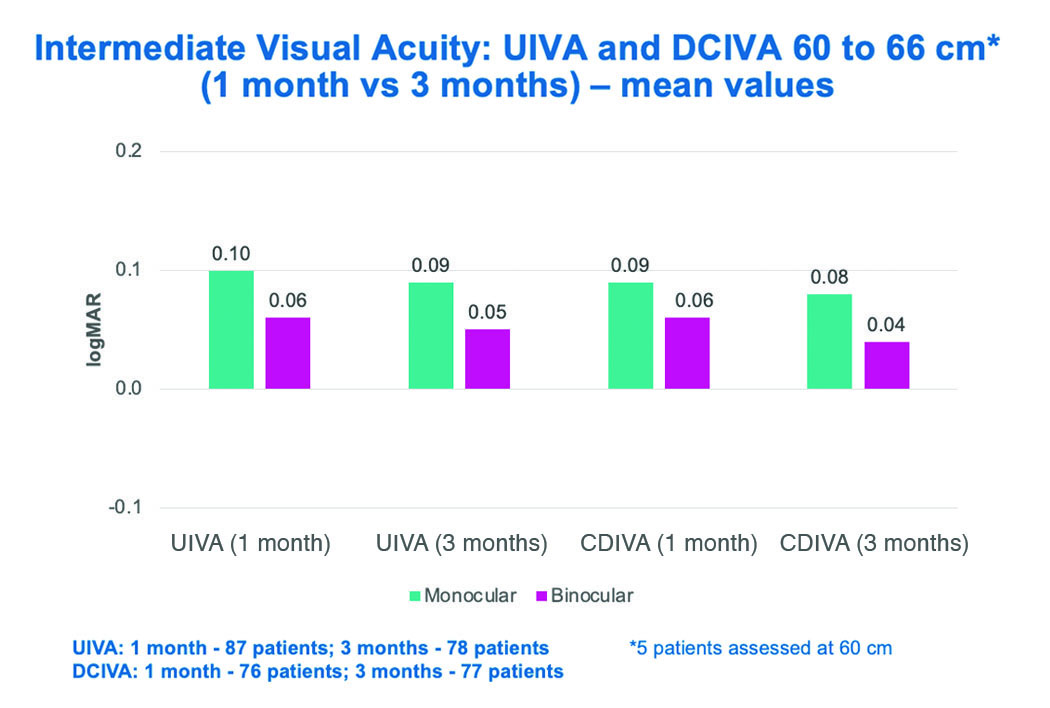
Figure 6. Mean values of uncorrected and distance corrected intermediate visual acuity at 1 and
3 months postoperative. Both UIVA and DCIVA improved from 1 to 3 months, showing very good
binocular DCIVA at 3 months.
UIVA: uncorrected intermediate visual acuity; DCIVA: distance corrected intermediate visual acuity
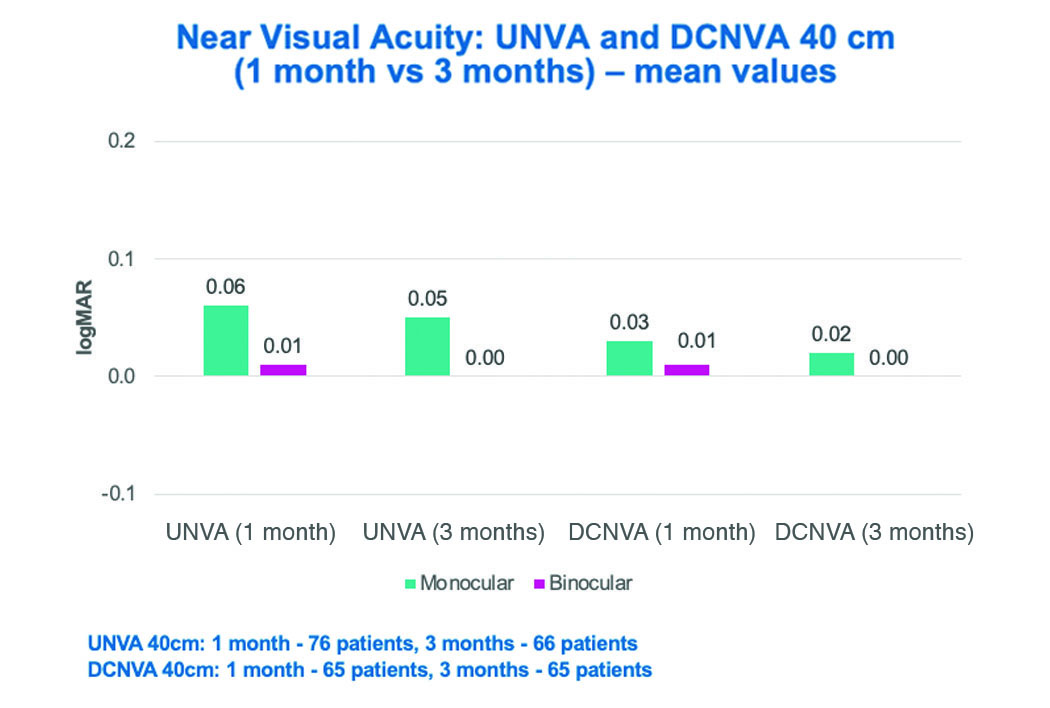
Figure 7. Mean values of uncorrected and distance corrected near visual acuity at 40 cm at
1 and 3 months postoperative. Both UNVA and DCNVA at 40 cm improved from 1 to 3 months, with
excellent near VA demonstrated binocularly.
UNVA: uncorrected near visual acuity; DCNVA: distance corrected near visual acuity
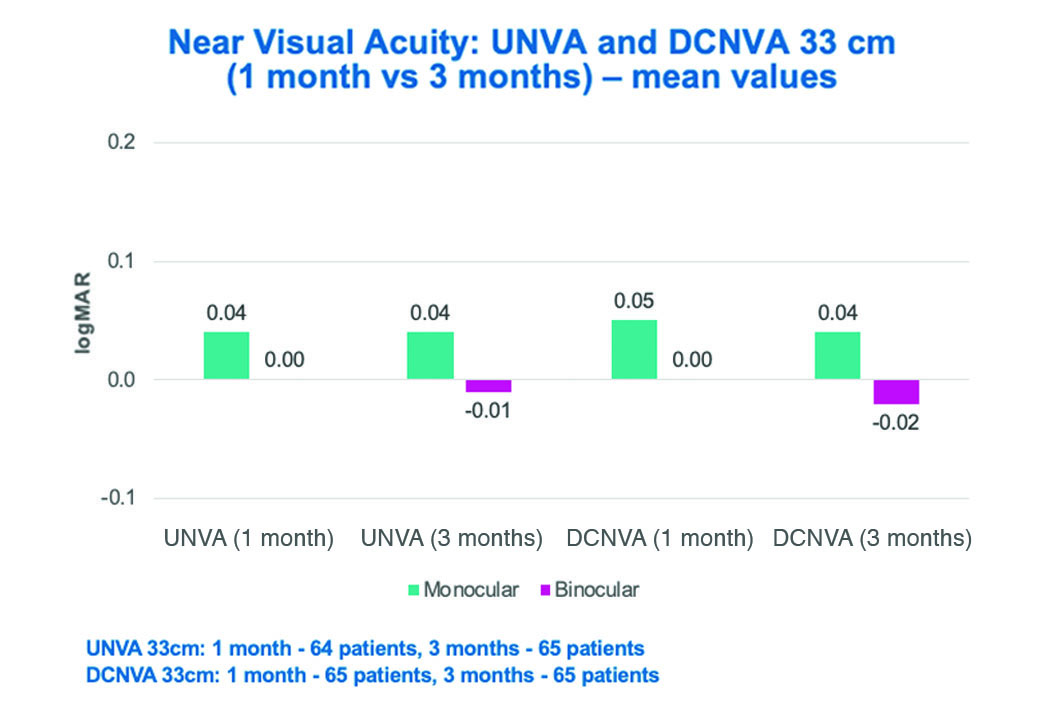
Figure 8. Mean values of uncorrected and distance corrected near visual acuity at 33 cm at
1 and 3 months postoperative. Both UNVA and DCNVA at 33 cm improved from 1 to 3 months, with
excellent near VA demonstrated binocularly.
UNVA: uncorrected near visual acuity; DCNVA: distance corrected near visual acuity
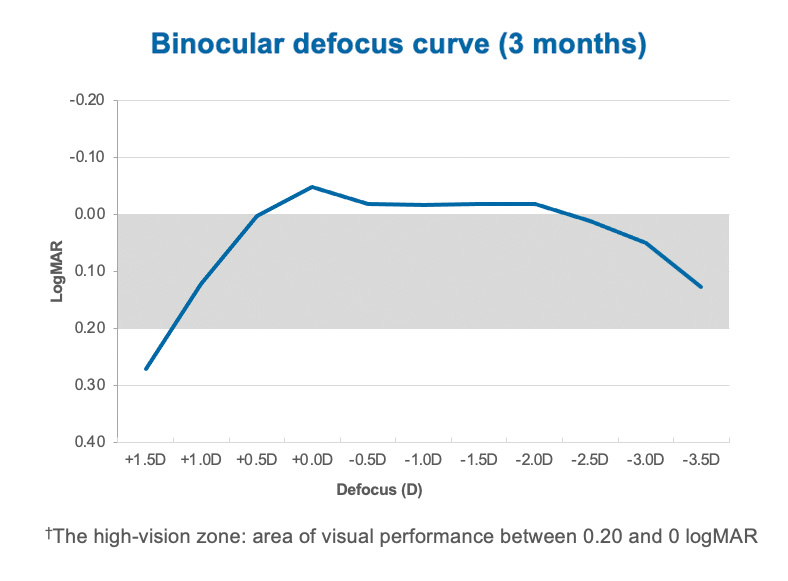
Figure 9. Extended depth of focus of 4.5 D in the high-vision zone† with excellent near VA at 40 and 33 cm. The binocular defocus curve shows excellent distance and intermediate vision, as well as continuous visual performance with no gaps from distance through near up to 30-35 cm.
According to the results of the quality of life assessment using the National Eye Institute Refractive Error Quality of Life 42 (NEI RQL-42) and the Spectacle and Light Dependence questionnaires, patients had a very high rate of satisfaction and a very high level of spectacle independence in different situations of everyday life and in various lighting conditions. This corresponds to the visual quality outcomes we have seen, as well as the rate of spectacle independence.
We all have excellent data to share. Dr. Caparas, please tell us about your personal experience with the WELL Fusion Optical System.
Victor L. Caparas, MD, MPH: Our study included 19 patients (38 eyes) with a mean age of 62 years. Surgeries were performed 1 week apart following the described protocol. In my patient population, more than two-thirds of the eyes were within ±0.25 D of intended correction at months 1 and 3, and 95% were within ±0.75 D of intended correction. As Prof. Auffarth mentioned, both the monocular and binocular uncorrected and corrected distance visual acuity at those time points was excellent (better than -0.1 logMAR), and there was a great improvement in uncorrected and distance-corrected near visual acuity at 40 and 33 cm (better than or equal to 0.0 logMAR). Both monocular and binocular uncorrected and corrected intermediate visual acuity at 60 cm was equal to or better than 0.1 logMAR at 1 and 3 months. With regard to the very flat defocus curve achieved with WELL Fusion, depth of focus was excellent, extending up to -3.50 D (30 cm) with visual acuity values consistently high at all distances (better than or equal to 0.0 logMAR). Also, there was a smooth transition from distance to near with no peaks or troughs. We were then able to bring the focus distance closer to 32 cm, which has not been shown with our previous clinical trials with the standard Mini WELL, and eliminate the gaps in near vision that are seen with some multifocal and trifocal IOLs.
Binocular contrast sensitivity measured at 1 m was higher than what can typically be achieved with trifocal and monofocal IOLs and with values even closer to a normal eye, which makes the WELL Fusion Optical System a very powerful option for cataract patients and those who desire a lens-based option for refractive surgery (Figure 10). The rate of glare and halos measured using the Halo and Glare Simulator software was very minimal and lower compared with diffractive multifocal IOLs, and all cleared by about 3 months postoperative (Figure 11).
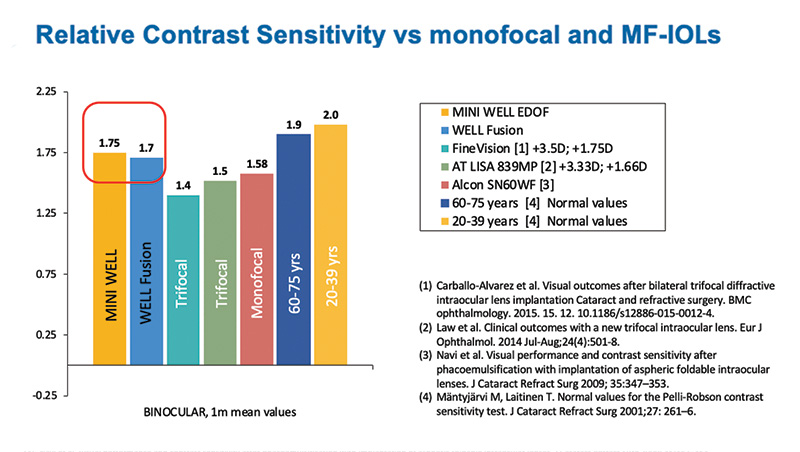
Figure 10. Binocular contrast sensitivity in Dr. Caparas’ center measured at 1 month. Higher values compared to both trifocals and monofocals and closer to normal values.
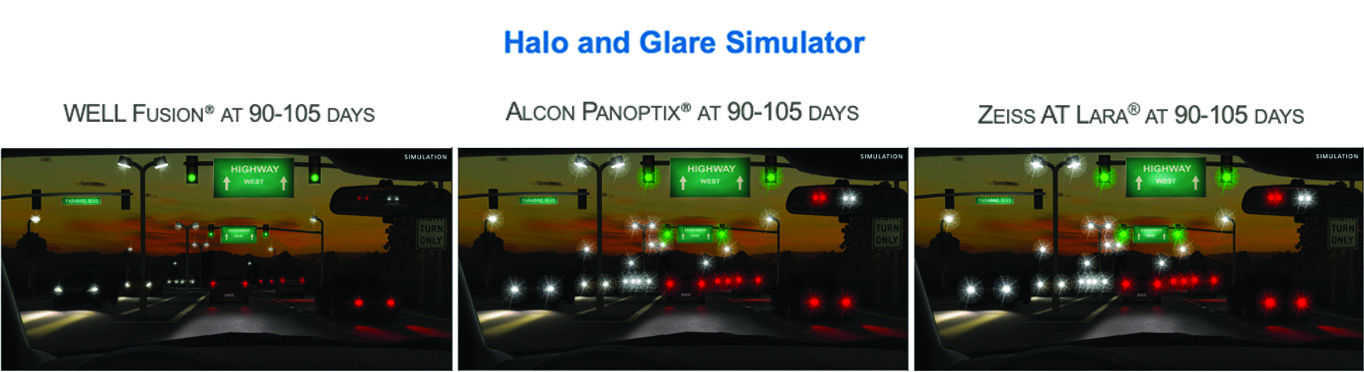
Figure 11. WELL Fusion halo and glare compared to the Alcon PanOptix and ZEISS AT LARA showing the very low level of WELL Fusion photic phenomena compared to diffractive multifocal IOLs.
Patients were asked about their rate of spectacle and light dependence with the WELL Fusion system, and the scores were outstanding. Overall, patients reported a near perfect satisfaction with a very low rate of spectacle use for tasks such as driving, watching television, using a laptop, reading numbers and words on a mobile device, and reading a book and newspaper. They also reported an extremely low rate of light dependence for the same tasks, confirming that the quality of vision was preserved. Finally, there are no changes in the surgical technique and pre-operative routine, which makes WELL Fusion a very good option for a surgeon.
Salvatore Cillino, MD, PhD: My results are very similar. A total of 10 patients (20 eyes) with a mean age of 65.7 years were enrolled in the study at my clinic. Thus far, I have preliminary results at 1 month. At that time, the binocular uncorrected distance visual acuity (mean values 0.01 logMAR) was better than the monocular uncorrected distance visual acuity, demonstrating that the two IOLs work together very well. Binocular uncorrected intermediate and near visual acuity also improved (mean values 0 and 0.01 logMAR respectively), the latter of which confirms the system’s ability to extend depth of focus across a broader range.
The vision-related quality of life, as evaluated by the NEI RQL-42 questionnaire, indicates an overall high satisfaction with the WELL Fusion in all groups of questions. The scores for glare and worrying about eyesight were lower with this system than with multifocal and trifocal IOLs (Figure 12). In my study I also performed contrast sensitivity, and values recorded were all within the normal range.
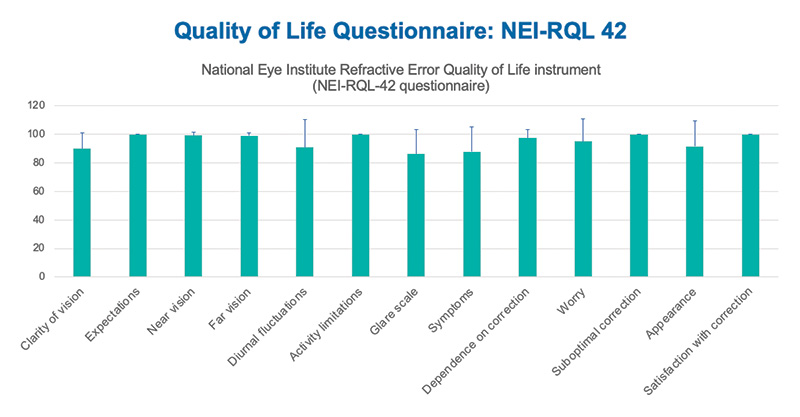
Figure 12. Very high patient satisfaction results from Prof Cillino’s study using the National Eye Institute Refractive Error Quality of Life 42 (NEI RQL-42) Questionnaire based on the assessment of vision-related quality of life.
We also tested patients’ reading performance using the MNREAD Test, which assesses reading acuity (RA), critical print size (CPS), maximum reading speed (MRS), and reading accessibility index. This test was performed at 40 cm. All values were within the normal range and were comparable to those recorded in our database of healthy eyes (patients between 30 and 40 years old).
From our results, I can confidently say that the WELL Fusion system provides patients with uninterrupted vision at all distances, excellent dynamic visual acuity and contrast sensitivity, and excellent reading ability at a variety of distances. Patients did not experience glare, halos, or dysphotopsias, and most achieved spectacle independence.
José Lamarca, MD, PhD: I enrolled 10 patients (20 eyes) as well, and 1- and 3-month results are available for nine of them. The mean age was 55.4 years. I like to perform a contact lens trial whenever possible so that the patient can experience how their vision might look after surgery.
As the others already mentioned, results with the WELL Fusion system were very good. About 86% of patients were within ±0.75 D of intended correction. The mean distance visual acuity was impressive. At this range, UCVA was better than 20/25 (0.1 logMAR) and BCVA was better than 20/20 (0 logMAR). Uncorrected intermediate visual acuity and distance-corrected intermediate visual acuity were greater than 20/25 and 0.1 logMAR binocularly, and this was stable from 1 to 3 months.
The most encouraging results were with near vision. Binocularly, the mean near UCVA was better than 20/25 (0.1 logMAR), and the mean distance-corrected near BCVA was 20/25 or better (0.1 logMAR). Overall, the WELL Fusion system extended patients’ depth of focus by 4.00 D, from 1.00 to -3.00 D, and contrast sensitivity values were very close to or better than the values of diffractive multifocal IOLs.
Our results confirm that continuous vision is achieved at all distances, with very good near vision (33 cm) with the WELL Fusion system. Our patients achieved a very high rate of spectacle independence at all distances and in different light conditions, and they were extremely satisfied with their postoperative outcomes (Figure 13). I think it’s a very encouraging system that will not trigger any negative surprises, such as those related to abnormal shape of the cornea or dry eye, which can be an issue with trifocals. These are situations that we would not want to deal with as ophthalmologists and that we do not want for our patients.
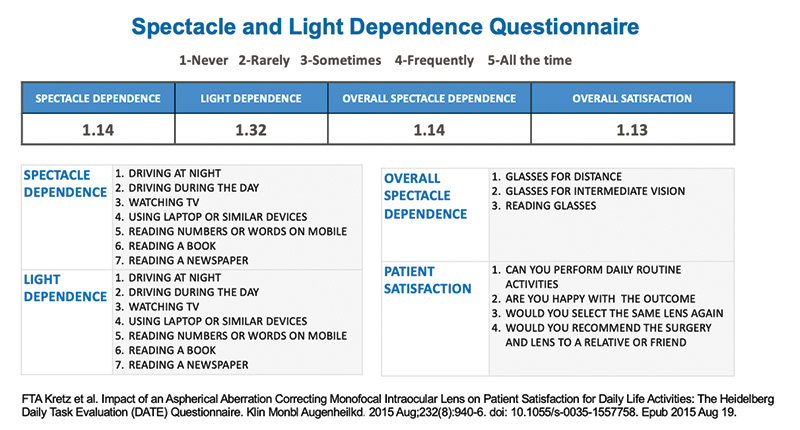
Figure 13. Very high patient satisfaction results from Dr Lamarca’s study using the Spectacle and Light Dependence Questionnaire.
Dorin Nicula, MD, PhD: For the purpose of this study, I have treated 20 patients (40 eyes) with a mean age of 54.6 years. I implanted Mini WELL in the dominant eye and Mini WELL PROXA in the nondominant eye. Surgeries were scheduled between 3 days and 1 month apart. In all eyes, total corneal astigmatism was less than 1.25 D, and the postoperative target refraction was less than 0.75 D. The Barrett formula was used with a constant of 1.75 and the Kane formula with a constant of 118.74, and the target was 0.30 D.
At 3 months, 85% and 95% of eyes, respectively, had a spherical equivalent of less than 0.50 and 0.75 D, demonstrating very good predictability with the WELL Fusion system. The refraction was stable between 1 and 3 months. Additionally, uncorrected and corrected distance visual acuity was stable between 1 and 3 months. At 1 and 3 months, binocular uncorrected distance visual acuity was better than 0.15 logMAR in 100% of patients. Regarding distance corrected binocular visual acuity, 100% of patients achieved better than 0.05 logMAR and 80% achieved 0 logMAR, at both 1 and 3 months. Uncorrected and corrected intermediate visual acuity improved between months 1 and 3. At month 1 follow-up, 85% of patients achieved a binocular uncorrected intermediate visual acuity of 0 logMAR; at month 3, 90% had achieved this. Binocular distance-corrected intermediate visual acuity was better than 0 logMAR in 85% of patients at month 1 and 95% at month 3.
Uncorrected and corrected near visual acuity at both 40 cm and 33 cm was excellent, even in low light conditions (Figure 14). At 1 month, for both distances, 85% of patients achieved a binocular uncorrected near visual acuity of 0 logMAR, and 100% of patients achieved better than 0.1 logMAR. At 3 months, 90% achieved 0 logMAR at 40 cm, 85% at 33 cm, and 100% achieved better than 0.1 logMAR at both distances. Binocular distance-corrected near visual acuity was also impressive. Both at 1 and 3 months, it was 0 logMAR or better in 95% of patients at both 40 cm and 33 cm. The binocular defocus curve with the WELL Fusion system was very flat and showed an impressive extended range of vision of up to 5.00 D and had a favorable defocus curve compared to other IOLs as shown in Figure 15. The WELL Fusion showed comparable visual acuity to trifocal IOLs at distance and 40 cm (-2.50 D) but with better visual acuity at 33 cm. A slight decrease in visual acuities was noticed between the main foci in trifocal IOLs, whereas the WELL Fusion presents a smoother curve indicating a stable and continuous very good visual performance at all distances. Additionally, the WELL Fusion system provided very good contrast sensitivity within the normal values, comparable to a monofocal IOL and to normal eyes.
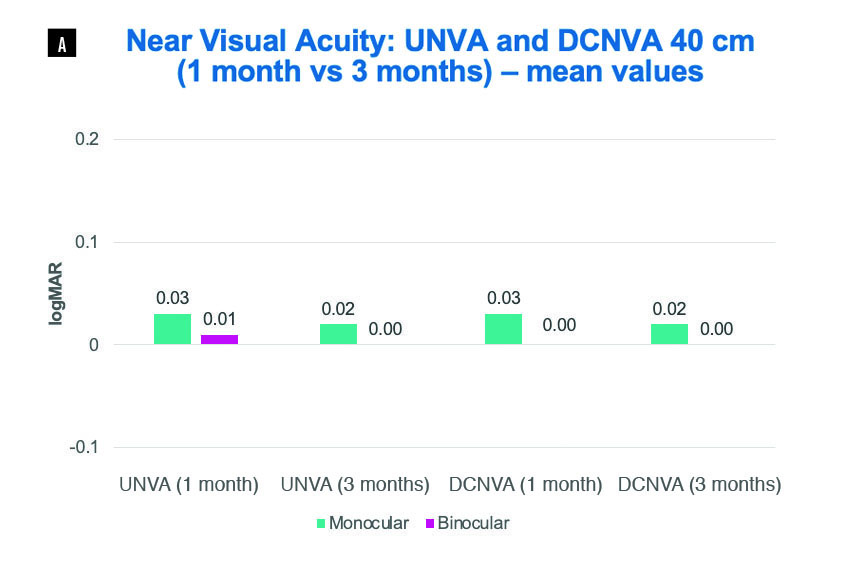
Figure 14A. Near visual acuity at 40 cm at Dr. Nicula’s clinic. Good near vision was reported even in
lower light conditions. UNVA binocular at both 1 and 3 months was better than 0.1 logMAR in 100% of
patients. DCNVA binocular at both 1 and 3 months was better or equal to 0 logMAR in 95% of patients.
UNVA: uncorrected near visual acuity; DCNVA: distance corrected near visual acuity
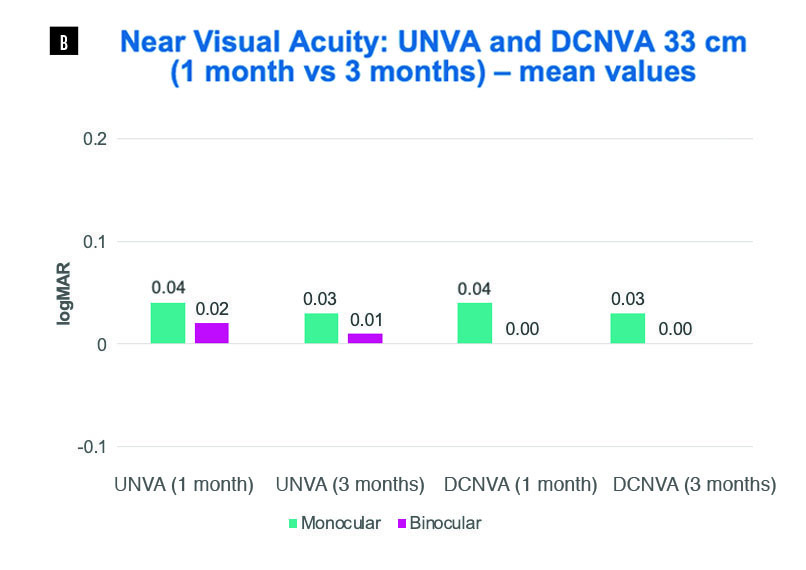
Figure 14B. Near visual acuity at 33 cm in Dr. Nicula’s clinic. Excellent near vision was reported. UNVA
binocular at both 1 and 3 months was 0 logMAR in 85% of patients and better than 0.1 logMAR in 100% of
patients. DCNVA binocular at both 1 and 3 months was better or equal to 0 logMAR in 95% of patients.
UNVA: uncorrected near visual acuity; DCNVA: distance corrected near visual acuity
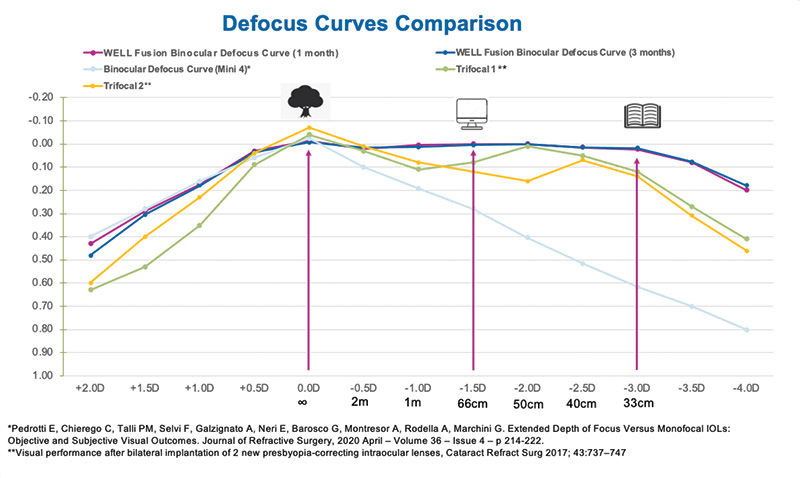
Figure 15. The very flat and smooth binocular defocus curve with the WELL Fusion system in Dr. Nicula’s study showing a great extended range of vision of up to 5.00 D without the gaps of trifocal IOLs.
Patients experienced a low incidence to no incidence of halos and glare using the Halo and Glare Simulator Software, and they reported a fast and easy neural adaptation process. There was a high rate of patient satisfaction, even for refractive lens exchange patients.
Emilio Pedrotti, MD, FEBO: My data is similar to that from others, which is encouraging because it shows that this system produces universal results. I have treated 10 patients (20 eyes) with a mean age of 75.2 years and have at least 1 year of follow-up. The target in all cases was emmetropia, comparing the SRK/T and Kane IOL formulas before choosing the IOL power.
All of my patients achieved excellent visual performance at distance, and both monocular and binocular uncorrected mean distance visual acuity improved from 0.18 and 0.12 logMAR, respectively, at 1 month postoperatively to 0.14 and 0.07 logMAR, respectively at 3 months postoperatively. The same was true for monocular and binocular corrected mean distance visual acuity, from 0.09 and 0.05 logMAR, respectively, at 1 month to 0.05 and 0.01 logMAR, respectively, at 3 months. We did not see any changes in the follow-up after 3 months.
Intermediate vision is very important for patients. Monocular and binocular uncorrected mean intermediate visual acuity at 60 cm improved from 0.10 and 0.06 logMAR, respectively, at 1 month to 0.09 and 0.02, respectively, at 3 months, as did monocular and binocular corrected mean intermediate visual acuity from 0.10 and 0.05 at 1 month postoperative to 0.08 and 0.04 at 3 months, respectively.
A similar trend was seen with monocular and binocular uncorrected and corrected mean near visual acuity at 33 cm. With respect to uncorrected, improvements were seen from 0.11 and 0.06 logMAR, respectively, at 1 month to 0.11 and 0.04 logMAR, respectively, at 3 months. For corrected, improvements were seen from 0.16 and 0.09 logMAR, respectively, at 1 month to 0.14 and 0.04 logMAR, respectively, at 3 months.
Patients achieved a visual acuity of 0.18 logMAR or better from 0.50 to -3.50 D, producing high vision at all distances. We measured contrast sensitivity under photopic, mesopic, and scotopic conditions in order to determine if there is any light dependence with these IOLs. Monocular and binocular contrast sensitivity is shown in Figure 16. All the values are within the normal range under all light conditions with good results, even after 1 month monocularly and improving with follow-up binocularly. Additionally, we performed Halometry (Aston) to objectively measure halos that patients can perceive. There was a very low amount of halos with the WELL Fusion, comparable to the amount seen in one of our studies with Mini WELL bilaterally implanted (Figure 17). Also, based on the results of the NEI RQL-42 Questionnaire, patients subjectively reported a negligible perception or no perception of halos confirming that halos are much less bothersome than with diffractive IOLs.
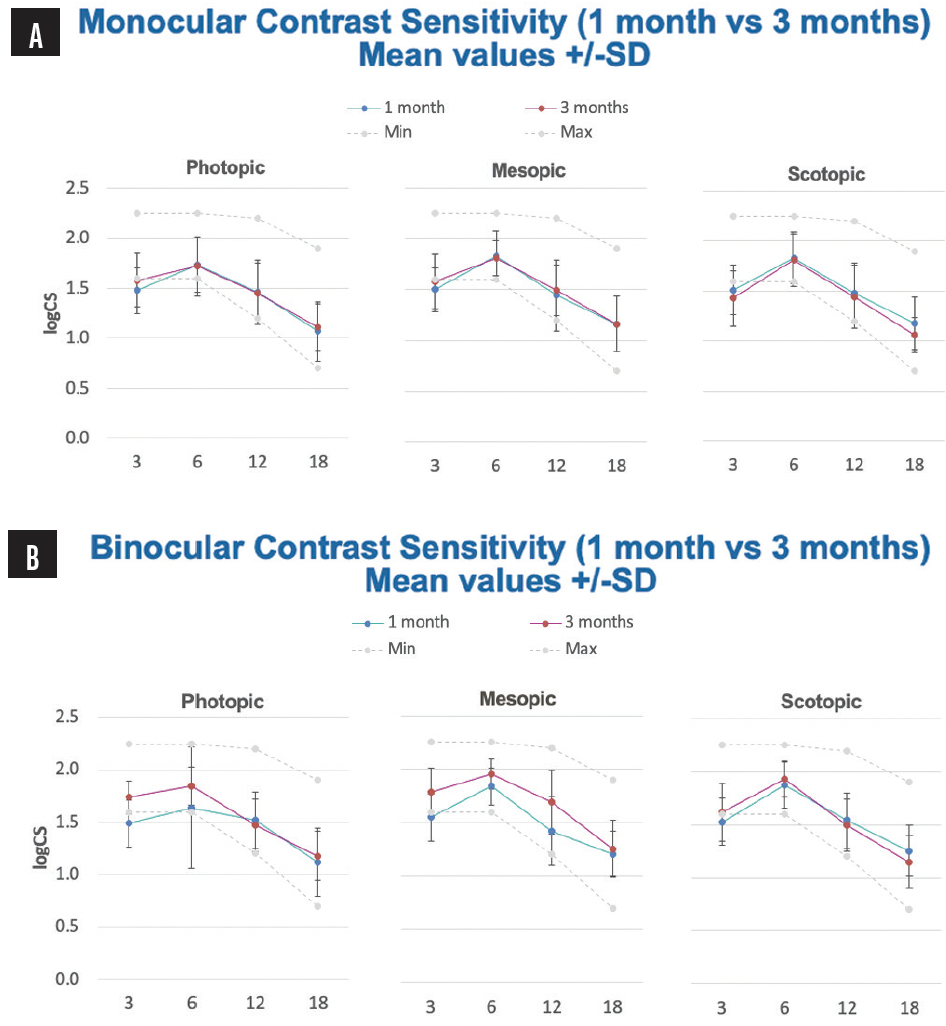
Figure 16. Prof. Pedrotti’s monocular and binocular contrast sensitivity at 1 month versus 3 months. Results showed no difference in contrast sensitivity compared to a monofocal IOL under all light conditions and a high level of contrast sensitivity improved during follow-up.
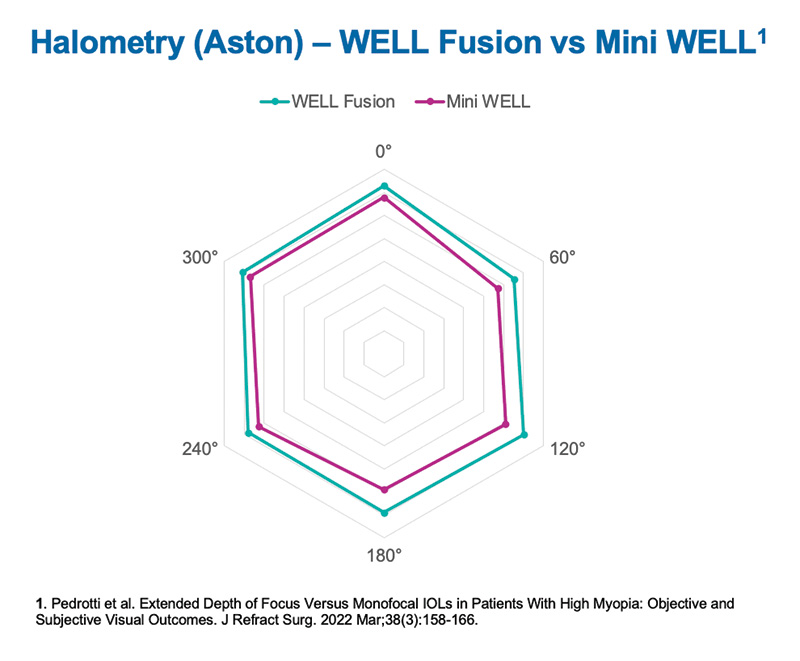
Figure 17. Prof. Pedrotti’s Halometry comparing WELL Fusion and a binocular implantation of Mini WELL IOL showing very similar results.
From my results with the WELL Fusion Optical System, I am confident that patients will achieve good visual performance at all distances, improving after neural adaptation (which is easier compared to different kinds of presbyopia-correcting IOLs), and excellent depth of focus up to 35 cm. One additional point that I want to make is that, whenever possible, the Mini WELL and Mini WELL PROXA should be implanted with a short period of time between procedures.
Sever Popa, MD, PhD: Like many of the other centers, my results are for 10 patients (20 eyes) who were binocularly implanted with the Mini WELL IOLs. Seven of the procedures were cataract surgeries, and three were refractive lens exchanges. The mean age of patients was 58.2 years. I used the Kane formula for IOL power selection, with a mean refractive target of 0.26 D (minimum, 0.18 D; maximum, 0.33 D).
The WELL Fusion system produced very good predictability, and at 3 month follow-up 100% of eyes were within ±0.50 D of the target refraction. The postoperative spherical equivalent improved from 1 to 3 months (Figure 18). Both uncorrected and corrected distance visual acuity also improved from 1 to 3 months, with all patients achieving 0.1 logMAR or better at 1 month and 0 logMAR at 3 months. Regarding uncorrected and corrected intermediate visual acuity, all patients achieved 0.1 logMAR uncorrected and 0.1 logMAR or better corrected, and 60% and 80%, respectively, achieved 0 logMAR at 1 month postoperative. At 3 months, all patients achieved 0.1 logMAR or better uncorrected and 0 logMAR distance-corrected intermediate visual acuity (Figure 19).
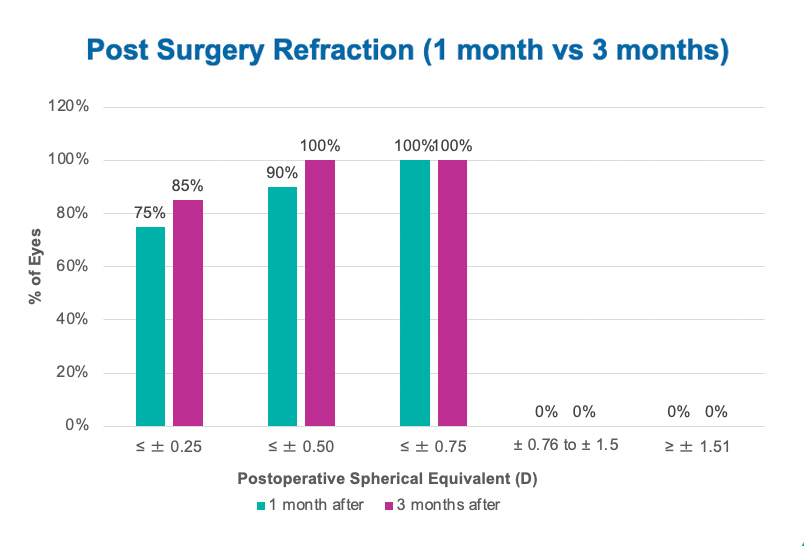
Figure 18. Post-surgery refraction at 1 month versus 3 months in Dr. Popa’s clinic. Results showed very good predictability. At 3 months, 100% of eyes were ≤ ±0.5 D.
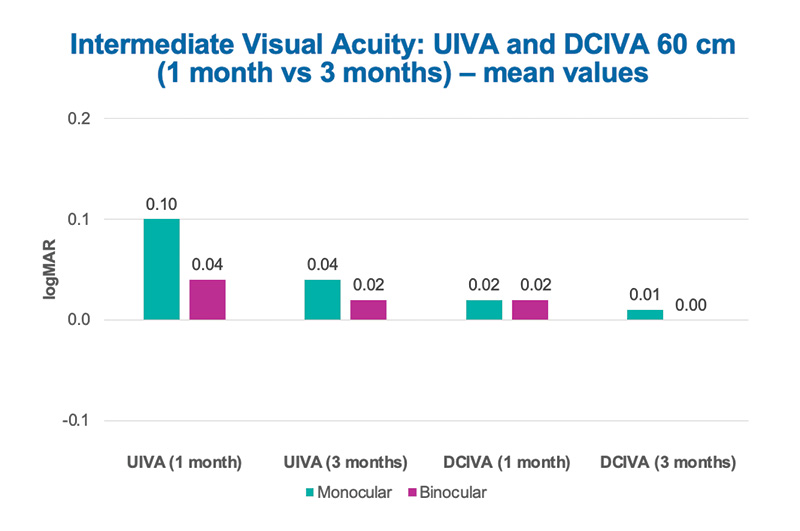
Figure 19. Intermediate visual acuity at 60 cm in Dr. Popa’s study. Both UIVA and DCIVA improved from 1 to 3 months. At 1 month and 3 months, UIVA was better or equal to 0.1 logMAR in 100% of patients. At 3 months DCIVA was 0 logMAR in 100% of patients.
Lastly, improvements were also seen with the near UCVA and BCVA at both 40 and 33 cm from 1 to 3 months. The binocular defocus curve also improved from 1 to 3 months, especially for reading distance, and there was a smooth and continuous visual performance with a visual acuity of 0.05 logMAR or better from distance to 40 cm (3.50 D defocus). At 3 months, patients achieved an extended depth of focus of 4.50 D in the functional vision zone (better than 0.2 logMAR) and excellent near vision at both 40 and 33 cm. We also compared the binocular defocus curve of the WELL Fusion system to the defocus curve in phakic patients, which shows a 5.00 D defocus for visual acuity of at least 0.1 logMAR. For WELL Fusion patients, they achieved 3.50 D defocus for a visual acuity better than 0.05 logMAR from +0.50 to -3.00 D and 4.50 D defocus for a visual acuity better than 0.2 logMAR from 1.00 to -3.50 D, indicating that the WELL Fusion closely matches the performance of the healthy human eye. Additionally, 100% of patients reported that they were spectacle independent, and none reported visual disturbances during follow-up.
Luca Vecchiarino, MD: My dataset includes results for eight patients (16 eyes) with a mean age of 62.9 years. The IOLs were implanted about 3 weeks apart. As others have mentioned, the WELL Fusion provides very high predictability. At 3 months, 93% of eyes were within ±0.25 D of the intended refraction, and 100% were within ±0.50 D.
The monocular distance visual acuity was better in the dominant eye at 1 month, but perfect fusion occurred by 3 months. At 3 months, the mean uncorrected and corrected distance visual acuity for monocular vision was 0.03 and -0.03 logMAR, respectively, and for binocular vision it was -0.03 and -0.07 logMAR, respectively. Monocular intermediate vision was very similar in both eyes with a functional improvement in binocular vision and very good stability from month 1. In fact, our results with mean uncorrected and distance-corrected intermediate visual acuity demonstrate that both were very similar.
Regarding near visual acuity at 40 cm and 33 cm, the results were better in the nondominant eye, with a great functional improvement in the binocular vision from the first month. Patients were immediately satisfied with their binocular near visual acuity and achieved spectacle independence.
The optical concept of WELL IOLs technology is to introduce controlled spherical aberrations of opposite signs into the central part of the IOL optics through concentric optical zones. This generates an elongated and continuous focus. In my experience, this concept provided a wider range of clear vision compared with the implantation of two standard extended depth of focus IOLs. We analyzed the spherical aberration with the Mini WELL PROXA with OPD SCAN at 3-, 4-, and 5-mm pupil sizes as compared to spherical aberration in normal eyes with a mean age of 29 years and at 4-mm pupil size. The results are shown in Figure 20. At all pupil sizes, the total internal spherical aberrations are always negative. This is very similar to a normal eye which demonstrates that the WELL Fusion is close to the natural vision of the human eye.
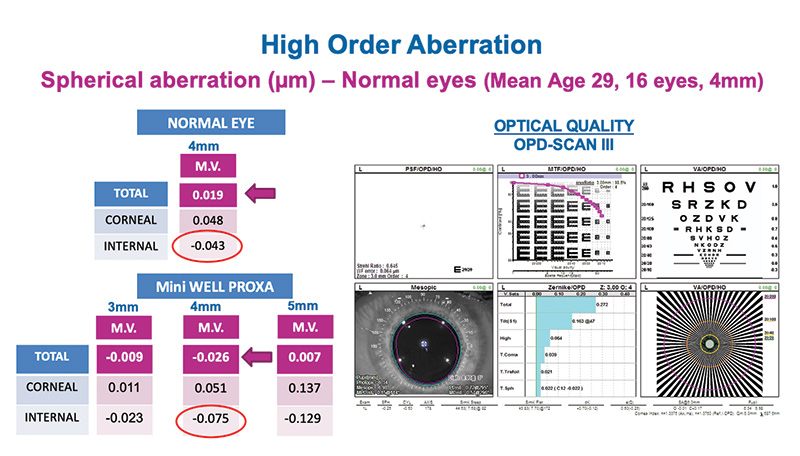
Figure 20. Dr. Vecchiarino’s aberrometry analyzing spherical aberration with Mini WELL PROXA and in normal eye at 4-mm pupil size. The total internal spherical aberrations of Mini WELL PROXA are very similar to a normal eye.
Prof. Auffarth: In my own personal experience with the WELL Fusion implanted in patients with retinal comorbidities, they experienced an improvement in uncorrected and corrected distance visual acuity, uncorrected and distance-corrected intermediate visual acuity, and uncorrected and distance-corrected near visual acuity at both 40 and 33 cm from 1 to 3 months postoperative. They also achieved excellent corrected distance visual acuity, binocular near visual acuity and very good binocular distance-corrected intermediate visual acuity at 3 months. Like the other panelists mentioned, my defocus curve was very flat, and the WELL Fusion provided continuous visual performance with no gaps in vision from distance to near up to 30-35 cm. The optical system extended depth of focus to 4.50 D in the high-vision zone (ie, intermediate) with excellent near visual acuity at 40 and 33 cm, providing full presbyopia correction also in patients with compromised eyes.
PATIENT SELECTION AND PREOPERATIVE CONSIDERATIONS
WELL Fusion is more forgiving than diffractive PC-IOLs and is suitable for a wide range of patients including post-refractive patients and patients with retinal pathologies like macular degeneration and glaucoma.
Prof. Auffarth: Who are the best candidates for the WELL Fusion Optical System?
Dr. Caparas: I broke my results down by age group (60 years and under, 61 to 65 years, and over 65 years). In terms of patient age, I advise my older patients to not expect to achieve the vision of a 35-year-old and to expect a longer neural adaptation process. Patients in younger age groups can expect to achieve sharp vision in most light conditions and a shorter neural adaptation process. This, however, is the same for any presbyopia-correcting IOL. In terms of satisfaction, older patients were just as likely as younger patients to recommend the procedure to their friends and family. I think the best candidates for the WELL Fusion Optical System are below the age of 65 years, professionals who work on a desktop computer, those who use smartphones regularly, and those who want to get rid of their glasses. WELL Fusion is also a nice option for patients over the age of 65 years who continue to lead an active lifestyle and still drive.
The WELL Fusion system is also appropriate for postrefractive surgery patients because of the little to no loss of contrast. I might not implant these lenses in patients who request refractive lens exchange, however, simply because they are highly demanding and expect very sharp vision at all distances.
Prof. Auffarth: Based on my experience, I would also consider extending the profile to include macular degeneration patients and those with glaucoma. In general, for older cataract patients who are used to wearing reading glasses, I have found that they are happy with the great defocus curve of the WELL Fusion.
Professor Cillino, would you perform your preoperative visit for the WELL Fusion differently than you would for a patient receiving diffractive IOLs?
Prof. Cillino: I would, yes. My approach has changed. Of course, I perform optical biometry, and I think SRK/T formula can be suitable for the majority of cases, even if I prefer the Barrett Universal II or Hoffer Q for short eyes, targeting a minimal hyperopia. Then I perform tomographic examination to evaluate corneal abnormalities or irregular astigmatism. Refractometry, tonometric and biomicroscopic evaluation with endothelial cell count are all part of my routine. I no longer perform pupillometry, which is different than what I do for diffractive IOLs. Generally speaking, I try to avoid pupils below 2 mm. Additionally, I do not check angle kappa because the technology is much more forgiving of large angle kappa.
Prof. Auffarth: Do you measure the corneal aberrations?
Prof. Cillino: I have some data for patients who underwent topography. It would be interesting to further investigate how corneal and IOL aberrations match, as it could help us explain some different results with the system.
Prof. Auffarth: I think this is not a prerogative like Dr. Vecchiarino showed in his results.
Dr. Vecchiarino: No, but I agree with Prof. Cillino, and I think it could be important to study aberrometry in the future.
Professor Pedrotti: I would add that keratometry measurements are crucial. In my previous studies with Mini WELL, I found that K readings (normal values, 43.50 D) were more predictive of postoperative results compared to the measurement of spherical aberrations. In particular, I found that eyes with more prolate corneas had better results than those with flatter corneas.
Additionally, I found that the Mini WELL works very well in eyes with high myopia (axial length up to 26.5 mm); this is not related to the corneal morphology, however, but to the axial length. I think that the combination of a lower-power IOL with a longer axial length can give us very good outcomes. Based on this, I also think that post-laser patients with myopic treatment may benefit from this technology.
Dr. Popa: I have been using the Kane formula for 2 years, which works well with both long and short axial lengths. For both Mini WELL and Mini WELL PROXA, I target around 0.30 D in order to achieve emmetropia and be more accurate with postoperative manifest refraction.
Dr. Lamarca: I also target 0.25 D.
It’s important to determine ocular dominance and guide patients through this process. Patients need to understand that it is a system that works binocularly.
Prof. Auffarth: This leads to the question of ocular dominance. Does it really matter in which eye these IOLs are being implanted?
Prof. Pedrotti: With this system, I think it’s important to define which is the dominant eye. With cataract patients, however, it can be challenging to determine. I am more confident to implant the Mini WELL PROXA in the eye with the least amount of visual acuity and the Mini WELL in the eye with the better performance prior to surgery. I implant the Mini WELL first, followed by implantation of the Mini WELL PROXA within 1 week.
Dr. Vecchiarino: In my experience, I found that patients implanted with Mini WELL first and then Mini WELL PROXA were happy with their near vision but can notice that, with the PROXA eye, the distance vision is not exactly the same as with the first eye with Mini WELL. For this reason, I decided to switch and start with surgery in the nondominant eye with the Mini WELL PROXA, and my patients are satisfied.
Prof. Auffarth: And how do you explain to your patients that they will receive two different IOLs?
Dr. Vecchiarino: I start by explaining that everyone has a dominant and a nondominant eye and that sometimes eyes require a different strategy to achieve good visual outcomes. There are two very similar IOLs that function differently for distance and near vision. Then, I explain to them that they do not have to try to test their vision with a single eye or compare one eye with the other. Patients need to understand that this is a system that works binocularly.
Prof. Auffarth: I usually tell patients that eye dominance is similar to being right- or left-handed, which everyone can understand, and most of the time, if you are right-handed, your right eye is your dominant eye. I like to have only 2 to 3 days between surgery on the two eyes. This way, patients don’t have time to differentiate between the eyes. I perform an eye-dominance test by asking patients to look through a hole and then switch it to their other eye. This can be an easier way for patients to understand which is their dominant eye.
Dr. Vecchiarino: I consider WELL Fusion as my first choice whenever patients express an interest in favoring near vision.
Neural Adaptation with the WELL Fusion
By Leonardo Mastropasqua, MD
Neural adaptation is the way in which the human brain adjusts to any kind of sensory input. After cataract surgery and implantation of diffractive, refractive, or a combination of diffractive and refractive multifocal IOLs, neural adaptation needs to be activated as the brain has to learn how to process the multifocal images on the retina, which are unfamiliar to the visual system. Only one of the images—corresponding to either the distance or to the near focal point—can be sharp, causing a dispersion of the light energy that enters the eye. When the brain fails to adapt to the new visual system, side effects such as the following are commonly experienced by patients: abnormal photic phenomena, dysphotopsias, and subjective perception of poor quality of vision (especially for distance) with no clear underlying reason.
Common reasons for neural adaptation failure include residual postoperative ametropia, especially astigmatism, higher-order aberrations, and the optical profile.
Extended depth of focus (EDOF) IOLs cause less photic phenomena compared to multifocal or trifocal IOLs because they have a more elongated defocus, translating to a more continuous range of near vision rather than multiple points of focus, but lack some near vision. Combining a trifocal and extended depth of focus IOL can be used to achieve increased spectacle independence, but this comes at the expense of quality of vision because of the risk for higher photic phenomena.
The Mini WELL and Mini WELL PROXA (both by SIFI ) share the same EDOF nondiffractive platform to create a continuous and extended focus without splitting light. These IOLs, which have complementary optical designs, can be used in combination to create a synergistic wavefront error between the two eyes that improves functional vision. The similar aberrometric pattern of the two IOLs avoids neural adaptation failure, thus ensuring continuous high-quality vision from distance to near up to 3.00 D—to achieve what we call natural functional vision.
SOME POSTOPERATIVE PEARLS
Prof. Auffarth: Let’s share some best practices for guiding patients through the postop process, including postop issues.
Dr. Popa: For any patients who are not satisfied after surgery, I evaluate the ocular surface for signs of dry eye disease. Most of the times, this is the culprit of their problems.
Prof. Auffarth: Dry eye treatment is important. What about refractive errors?
Prof. Cillino: Refractive errors are rare with the WELL Fusion system. This also depends on the Mini WELL EDOF concept, which is based on the distribution of spherical aberrations generating an extended continuous focal point. This can overcome small errors, differently than with diffractive IOLs, because of their multiple discrete foci.
Dr. Nicula: I agree, I didn’t have any big refractive errors after surgery that couldn’t be solved with a pair of glasses for night driving. Also, I prescribe all patients over the age of 65 years artificial tears to use for the first 6 weeks after surgery.
Prof. Auffarth: Patient guidance is important. One thing I’ve noticed is that patients often focus mainly on a certain distance. When they come in for their follow-up exams, I say, “You did a great job adapting for the near and intermediate focus, but you have to concentrate a bit more on distance. Take your dog on a walk and look in the distance, for example. When you do office work, get up every hour and look outside.” I get the impression from patients that this strategy helps them achieve more balanced vision. We have to educate patients and guide them through the process to avoid complaints.
CONCLUSION
Prof. Auffarth: To summarize, the WELL Fusion system provides patients with perfect results. Based on our collective experiences, we can say that WELL Fusion represents the best functioning system to achieve an excellent defocus curve with an elongated focus of vision for distance, intermediate, and near at no expense in terms of dysphotopsia. Visual quantity and quality are extremely balanced here. Our next challenge is to extend the use of this technology to other patient profiles. I look forward to continuing our work by publishing data and speaking to our colleagues at conferences about the WELL Fusion technology.
1. The Fundingsland Group. 2020 CRST Clinical Survey of 450 cataract and refractive surgeons. October 2020.
2. De Vries NE, Nuijts RM. Multifocal intraocular lenses in cataract surgery: literature review of benefits and side effects. J Cataract Refract Surg. 2013;39(2):268-278.
3. Pedrotti E. First clinical experience with the optical system WELL Fusion (Mini WELL + Mini WELL PROXA). Webinar: A new dimension in the correction of presbyopia; December 12, 2020.
4. Mastropasqua L. First implants and clinical results with the optical system WELL Fusion (Mini WELL + Mini WELL PROXA). Webinar: A new dimension in the correction of presbyopia; December 12, 2020.










This supplement reflects the views and clinical experiences of the experts participating in this meeting and does not reflect information from formal clinical studies.



