
Trifocal IOLs have become a popular option with patients because of their potential to enhance visual quality at near, intermediate, and distance. All trifocal IOLs follow the same basic principle, which is to combine two diffractive step-widths to create near, intermediate, and distance foci. Each trifocal lens is unique in its design details, and slight variances exist in their safety and efficacy.
I conducted a small study comparing performance outcomes with two diffractive trifocal IOLs, the AT LISA tri (Carl Zeiss Meditec) and the AcrySof PanOptix (Alcon). This article overviews my results.
BACKGROUND
The AT LISA tri has a central diffractive trifocal zone. It has covering all distances and an outer bifocal zone to enhance distance and near vision under low light conditions. The intermediate and near focus planes are 80 cm and 40 cm, respectively. The light distribution is 50% for distance, 20% for intermediate, and 30% for near. The PanOptix IOL, which has a central diffractive trifocal zone and an outer refractive distance zone, has similar light distribution, with 50% for distance and 25% for each intermediate and near. The intermediate focal point of the PanOptix is 60 cm and the near focal point is also 40 cm.
We recently conducted a single-center, prospective study to determine the performance outcomes of the AT LISA tri and AcrySof PanOptix IOLs. Twenty-eight patients were included in the study, 13 in the AT LISA tri group and 15 in the PanOptix group. All patients underwent routine cataract surgery or refractive lens exchange to target emmetropia, and the Barrett Universal II formula was used for IOL power calculation.
Patients in both groups had similar axial lengths, mean keratometry readings, and corneal astigmatism. There was a slightly higher incidence and range of anterior corneal astigmatism in the AT LISA tri group.
STUDY OUTCOMES
The results discussed here are from 3 months postoperative. Generally speaking, the two lenses performed very well. The refractive outcomes were similar between the AT LISA tri and PanOptix groups in terms of sphere and spherical equivalent (mean spherical equivalent, -0.053 D vs 0.042 D, respectively). However, the AT LISA tri provide slightly superior distance visual acuity as well as intermediate visual acuity at 70 cm.
In terms of patients’ functional vision (Figure 1), when we looked at monocular distance UCVA, about 70% of all patients achieved 6/6, with slightly better values in the AT LISA tri group (69%) compared to with the PanOptix group (63%). Nearly 100% of patients achieved 6/7.5 and 6/9.5. Results for monocular distance BCVA were similar.
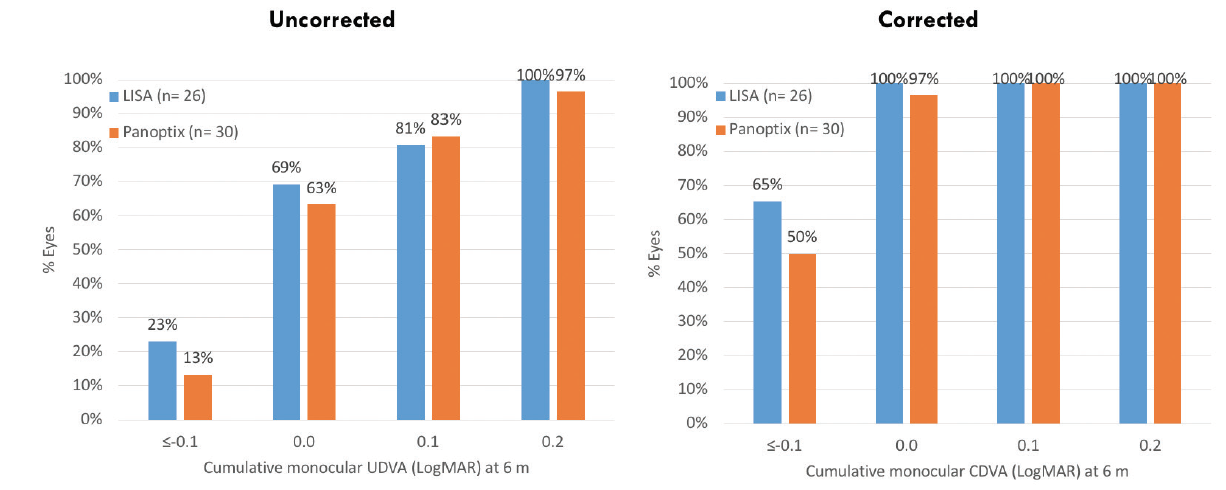
Figure 1. Uncorrected and corrected distance visual acuity with the AT LISA tri and PanOptix IOLs.
We also compared intermediate vision with the lenses, selecting a midpoint of 70 cm to achieve a head-to-head comparison. In the AT LISA tri group, nearly 80% of patients had excellent (0.0) uncorrected intermediate visual acuity, compared with 60% in the PanOptix group (Figure 2). The latter improved at the manufacturer-specified distance of 60 cm. When we looked at the near data at 40 cm, again both lenses did very well, with all patients achieving N 4.5 (Figure 2). Presbyopic patients in the study were among the most satisfied with this gain in near visual acuity.
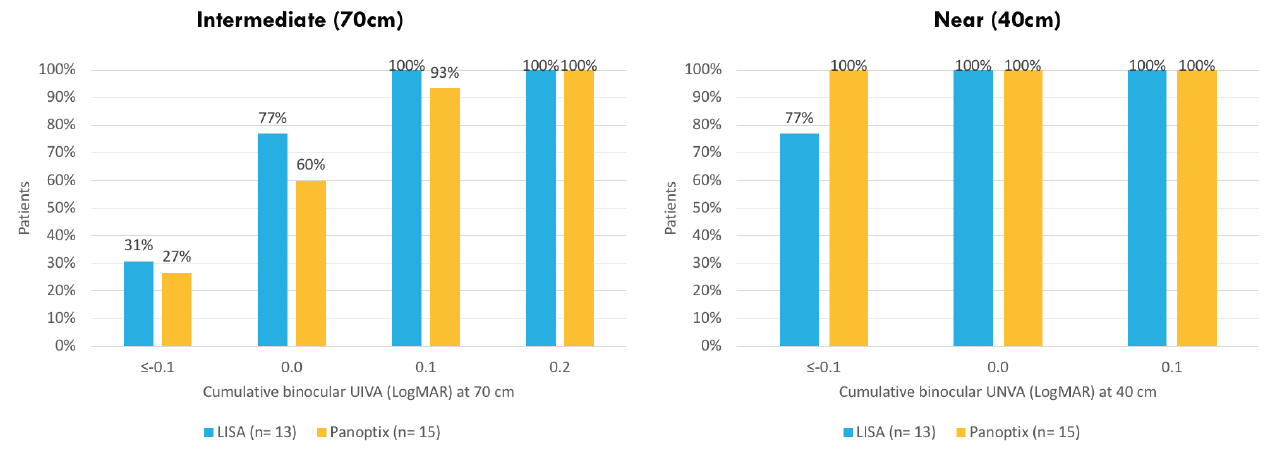
Figure 2. Binocular uncorrected intermediate and near visual acuities with the AT LISA tri and PanOptix IOLs.
Refractive outcomes were comparable to those in other published studies. About 90% of all patients enrolled in the study were within ±0.50 D of the target refraction, and 60% to 70% were within ±0.25 D. Both lenses did very well in terms of toric accuracy and residual cylinder; again about 90% of patients in both groups were within ±0.50 D.
PATIENT SATISFACTION
Also, both groups achieved a very high level of spectacle independence for distance, intermediate, and near vision. The only difference between the two lenses seemed to be for intermediate vision, and in our study a larger percentage of AT LISA tri patients compared with PanOptix patients achieved 0.0 uncorrected intermediate visual acuity (80% vs 60%, respectively) at 70 cm. It is therefore important in choosing the appropriate IOL for a patient that their intermediate distance requirement be considered.
An overwhelming majority of patients in both groups (90%) were completely or very satisfied with their postoperative vision, and 95% said they would choose the same IOL again. Further, more than 90% of patients would recommend the lens they received to family or friends.
Also factoring into patient satisfaction was the low incidence of halos and glare in each group. When asked about the occurrence of halos and glare, 100% of AT LISA tri patients responded that they never or only occasionally experienced glare.
TAKE-HOME POINTS
There are three points that we learned through this study.
No. 1: Aim for zero refractive error. In particular with trifocal IOLs, it is important to minimze refractive errors in order to achieve optimal distance vision.
No. 2: Good light is crucial for near and intermediate vision tasks. Trifocal IOLs split the light into three focus planes, making only a fraction of the light effectively available for different focus distances. Patients must therefore be educated that they may need sufficient light for certain tasks, such as reading without spectacles at near or intermediate distances.
No. 3: When selecting a trifocal IOL, it is best to consider the patient’s intermediate distance requirements. For instance, the AT LISA tri is a great choice for individuals who do a significant amount of office work, as computer desktops are typically located at a distance of around 70 cm.
CONCLUSION
As shown in our study, both lenses provide patients with good outcomes. The key difference, however, was in intermediate vision at 70 cm, with more patients in the AT LISA tri group achieving 0.0 uncorrected intermediate visual acuity. The AT LISA tri also provided slightly superior distance visual acuity, and our result is in line with previous studies.1 Both lenses provided excellent near visual acuity, with a slight advantage with the PanOptix.
In my personal experience, AT LISA tri patients experience a spectacular wow factor the day after surgery, with most reporting a drastically enhanced clarity of vision and seamless vision. The difference in optical quality, based on the material and optical concept of the AT LISA tri, as well as my patients’ positive outcomes, have confirmed in my mind that this lens is the best choice for even my most demanding cataract surgery and refractive lens exchange patients.
We must always consider patients’ visual requirements when selecting the appropriate IOL. I am confident when recommending the AT LISA tri IOL because it provides excellent distance, intermediate, and near visual acuities, and it offers a high level of spectacle independence. In my experience, this lens is a reliable solution to achieve excellent patient satisfaction.
Get in touch for more information!
1. Böhm M, Hemkeppler E, Herzog M, et al. Comparison of a panfocal and trifocal diffractive intraocular lens after femtosecond laser–assisted lens surgery. J Cataract Refract Surg. 2018;44:1454-1462.



