
Transitioning from cataract surgery to refractive cataract surgery—where the focus shifts to postoperative refractive accuracy—requires commitment, but it is one that any ophthalmologist can make when time is taken to understand the available lens-based refractive correction options and how to best utilize them for their patients. This article will focus specifically on trifocal optics and include discussion on patient selection and education and long-term outcomes with the AT LISA tri (Carl Zeiss Meditec).
PATIENT SELECTION
The most important consideration in refractive cataract surgery is patient selection. You must take time to focus on each individual patient by getting to know his or her specific visual requirements, lifestyle needs, and personality type. Some patients are focused on near tasks such as reading or handcrafting. Others desire optimized intermediate focus for computer work. And of course others want an overall excellent quality of vision without spectacle correction. Likewise, consider the light conditions that patients typically work under.
Individualized treatment is the key to success with refractive cataract surgery. Ask your patients the following questions:
- How much spectacle independence do you require?
- How accepting would you be of dysphotopsias?
- What distance or distances of vision are most important to you in your daily life?
- What light conditions do you typically work in or perform your hobbies in?
You must also diagnose and treat any ocular surface disease before proceeding with refractive cataract surgery, as its presence will not only affect preoperative measurements and IOL power calculation but also complicate the healing process and influence postoperative outcomes. Patients with severe, uncontrolled dry eye disease and those with a concomitant disease that limits visual outcomes are contraindications for a trifocal IOL.
When transitioning to refractive cataract surgery with trifocal IOLs, the easiest patients to start with are presbyopic hyperopes. Emmetropes, on the other hand, can be difficult because they may lose some distance vision.
SETTING EXPECTATIONS
The second most important aspect of refractive cataract surgery is setting the right expectations with your patients. Most of our cataract patients are used to a high level of glare due to the opacification of the crystalline lens, but they won’t be used to halos. Instead of highlighting the possibility that they could experience halos with a trifocal IOL, emphasize to them that their focus will be sharper and that they will no longer experience glare. You must mention that halos are possible, but lead with those other points I just mentioned. Also, explain to patients that this lens will better compensate for their overall vision.
I also find it helpful to use a halo and glare simulator. Patients are shown images with average values of halos and glare and are asked, “Can you live with it? Do you think that would bother you?” And usually patients are happy to exchange that glare for some halos. Explain to patients that they will need good light, especially if they want to do near tasks under dim light conditions, and that there will be a period of neural adaptation while their brain learns the new optical system. I always try to underpromise and overdeliver. (Editor’s note: For more pointers on talking to patients and explaining the AT LISA tri surgical experience, see Dr. Daponte’s article on pg 10.)
LONG-TERM STABILITY
We recently performed a 3-year follow-up study to determine the functional outcomes with the AT LISA tri and the AT LISA tri toric. The study enrolled 109 men and 142 women with high myopia and high hyperopia with significant astigmatism. The median age was 62 years.
The refractive results with the AT LISA tri are found in Table 1. The results with the toric version at 2 years, found in Table 2, were similar. What we found is that both lenses had excellent functional results and long-term stability (Figure). UCVA for distance, intermediate, and near vision stayed the same over the 3-year period with the AT LISA tri and a 2-year period with the AT LISA tri toric.
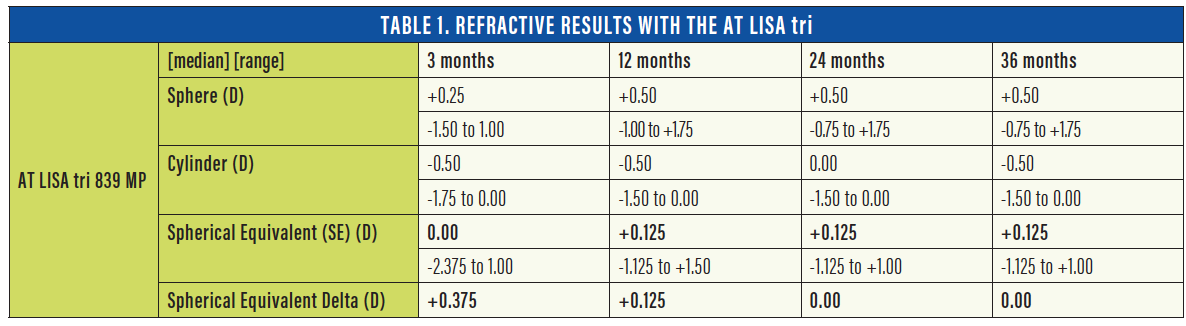
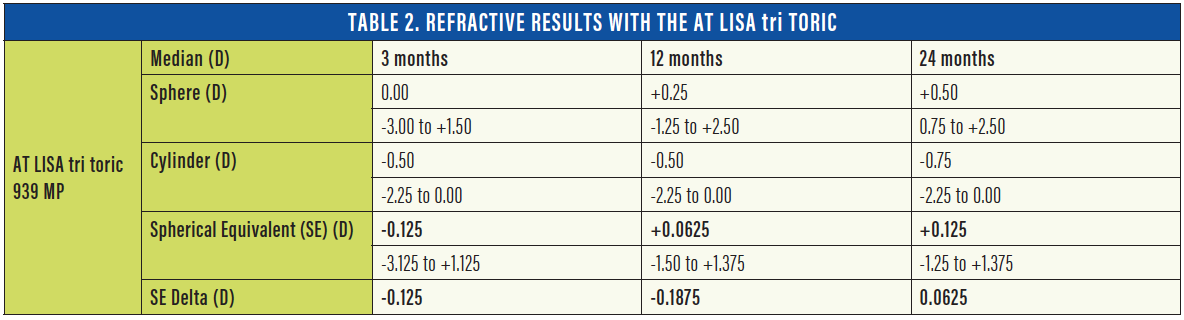
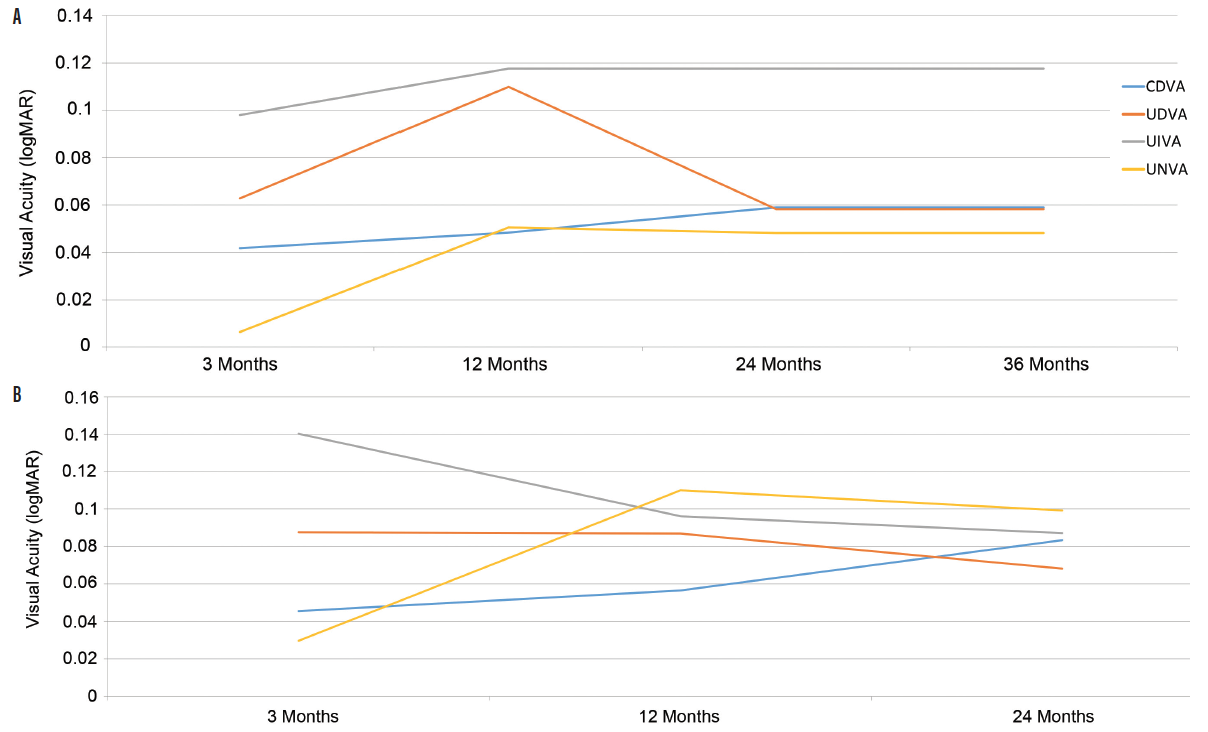
Figure. Functional results with the AT LISA tri (A) and AT LISA tri toric (B).
CONCLUSION
The AT LISA tri and tri toric expand the range of patients in whom I can safely and effectively perform refractive cataract surgery. Further, the long-term outcomes with this lens are excellent, and there is a high level of patient satisfaction. For those surgeons who are ready to transition to refractive cataract surgery, a great place to start is with the AT LISA tri IOL.
Get in touch for more information!




