
Sponsored by Carl Zeiss

Paola Piccinini, MD
Centro Oculistico Sardo
Sassari, Italy
If left untreated, epithelial ingrowth can lead to irregular corneal astigmatism—which may decrease visual acuity—or cause the spread of epithelial cells into the visual axis.
Although there is a need for further research into the risk factors of SMILE and epithelial ingrowth, there are findings related to LASIK and epithelial defects at the time of surgery that connect the complication to a history of recurrent corneal erosions, corneal basement membrane epithelial dystrophy, ingrowth in the opposite eye, and Type I diabetes. These findings provide some insight into how to approach this complication after SMILE.1
CASE PRESENTATION
A 40-year-old woman underwent small incision lenticule extraction (SMILE) treatment for low myopia and moderate myopic astigmatism. During the treatment of the left eye, a suction loss occurred after the refractive cut and the lenticule side cut were performed. As per protocol, I did an immediate restart and the laser treatment was finished by cutting the upper part of the lenticule and the incision cut. However, I slightly decentered when I was redocking the contact glass. As a result, the incision cut and lenticule cut were very close to each other leaving only a small clearance zone. Due to the small clearance, I was worried that I might enter the lower plane instead of the upper plane first, so I reentered the small incision several times to ensure that I would find the entrance for the upper plane. Thereby, an epithelial defect was created and, due to reentering the instrument repeatedly, some epithelial cells were pushed under the cap.
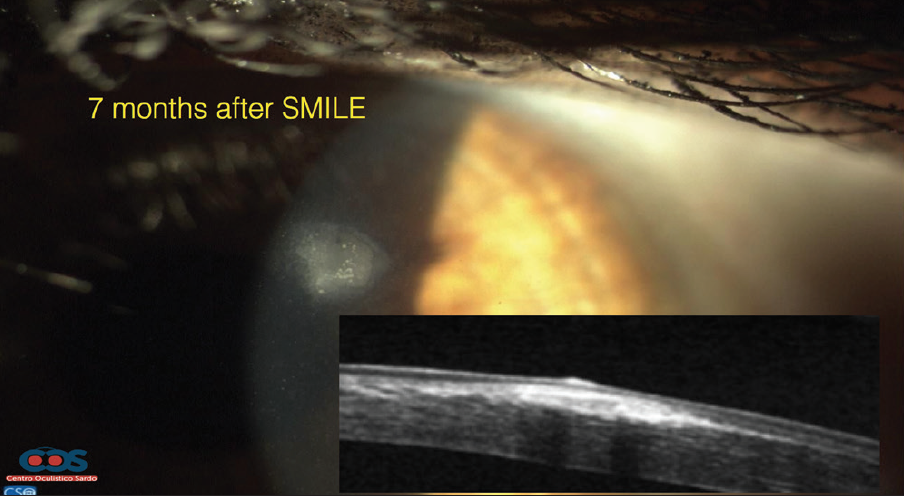
Figure 1. OCT imaging shows epithelial cells and hyper-reflectivity 7 months after SMILE was performed.
After one week, I discovered the epithelial ingrowth. Since the patient did not have any symptoms and her vision was 20/20, I decided to observe the growth over time, and I examined the patient during follow-up visits at 7 days, 20 days, 2 months, 4 months, and 7 months after the procedure. During the 7-month follow-up visit, I noted that the epithelial ingrowth had thickened and the cap appeared thinner. I decided to evaluate the available treatment options.
TREATMENT OPTIONS
After reviewing the case with my colleague, I observed two treatment options: manual removal and Neodymium: Yttrium-Aluminum-Garnet (Nd:YAG) laser treatment. During manual removal, the epithelial ingrowth is scraped from the stromal bed and underneath the flap/cap. However, studies have shown that the recurrence rate of epithelial ingrowth after manually scraping the cells is high.2 I decided against manual removal because the patient’s visual acuity was excellent. Manual removal has, as a surgical procedure, a potential risk for infection. Since the patient was asymptomatic and had good visual acuity, I decided for a less invasive treatment option.
Nd:YAG laser treatment induces a cavitation within the interlamellar space, causing collateral tissue destruction where the epithelial nests are located and consequently destroying the epithelial cells. Literature shows that epithelial ingrowth treated with Nd:YAG laser is an easy and effective treatment for epithelial ingrowth after LASIK. In one study published in the American Journal of Ophthalmology in 2015, Ayala, et al, treated 30 eyes with Nd:YAG laser for clinically significant epithelial ingrowth that developed following LASIK. After the Nd:YAG laser treatment, the opacities caused by the epithelial ingrowth disappeared in 80% of the cases. In 40% of the cases, two or more sessions of Nd:YAG laser treatment were necessary to eliminate the epithelial ingrowth areas entirely. Furthermore, in 60% of the cases, visual acuity improved by one or more lines of vision and the corneal topography was more regular. Patients’ symptoms, like glare and halos, also improved in all cases. Researchers adjusted the intensity of the laser in each case to focus directly on the epithelial ingrowth areas.3,4
TREATMENT AND OUTCOME
I decided to move forward with treating the epithelial ingrowth with Nd:YAG laser. Ayala et al3 recommended using an intensity of 0.6 mJ of the spots with the Nd:YAG laser. However, in 2015 researchers found that flap melting after Nd:YAG laser may have been caused by using too many spots in the same session.4 In this study, researchers did not delay the treatment as Ayala et al did. Considering these findings, I decreased my power to 0.3 mJ so that I could see the bubbles inside of the tissue. I applied 12 shots at 0.3 mJ, focusing on the interface. Seven days after Nd:YAG laser treatment was performed, the patient’s epithelial ingrowth reduced, and 14 days after Nd:YAG laser, OCT imaging showed only amorphous material. After 3 months, OCT imaging showed only a ghost image of the ingrowth.
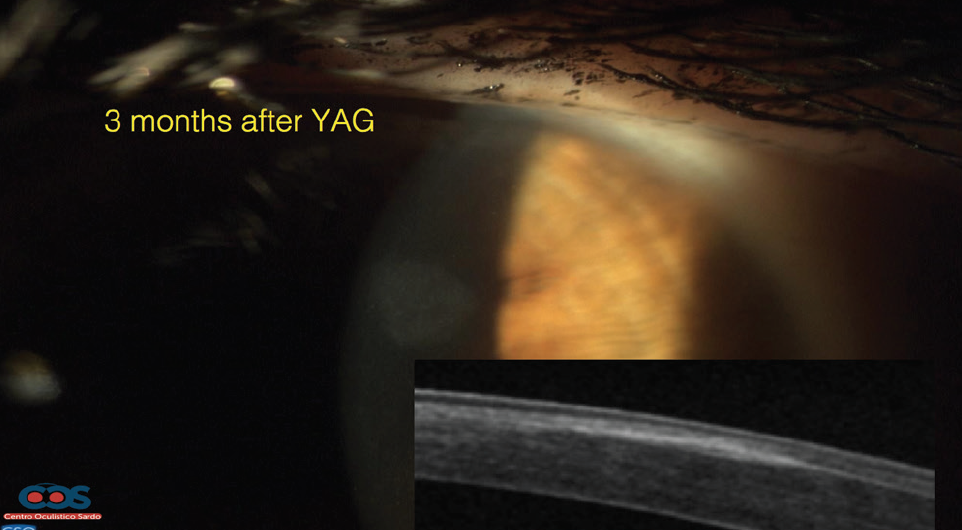
Figure 2. OCT scan before Nd:YAG laser, 14 days after Nd:YAG laser, and 3 months after Nd:YAG laser.
CONCLUSION
Even if epithelial ingrowth after SMILE is highly unlikely due to the small incision, it can still occur in rare cases. However, risks can be reduced by minimizing manual manipulation as much as possible to avoid spreading epithelial cells underneath the cap and creating epithelial defects. Epithelial ingrowth can be further reduced by evaluating the patient’s history of recurrent corneal erosions, corneal basement membrane epithelial dystrophy, and type I diabetes. If, despite all precautions, a surgeon faces a case of epithelial ingrowth after SMILE, Nd:YAG laser may be an effective treatment and resolution.
1. Kim JM, Goel M, Pathak A. Epithelial ingrowth - Nd:YAG laser approach. Clin Exp Ophthalmol. 2014 May-Jun;42(4):389-90.
2. Wang MY, Maloney RK. Epithelial ingrowth after laser in situ keratomileusis. Am J Ophthalmol. 2000 Jun;129(6):746-51.
3. Ayala MJ, Alió JL, Mulet ME, De La Hoz F. Treatment of laser in situ keratomileusis interface epithelial ingrowth with neodymium:yytrium-aluminum-garnet laser. Am J Ophthalmol. 2008 Apr;145(4):630-634. doi: 10.1016/j.ajo.2007.11.022. Epub 2008 Feb 1.
4. Kucukevcilioglu M, Hurmeric V. Localized flap melt after Nd-YAG laser treatment in recurrent post-LASIK epithelial ingrowth. Arq Bras Oftalmol. 2015. Jul-Aug;78(4):250-1.
