
Sponsored by Oculentis

When multifocal IOLs were introduced in the late 1980s, all were designed with a rotationally symmetric profile and were either based on the principle of diffraction or refraction of light or on a combination of those two principles. Regardless of the unique design of any particular multifocal IOL, the overarching idea was that multifocals could potentially provide patients with an opportunity to achieve spectacle independence and better quality of vision over a range of distances, rather than at just one distance like monofocal IOLs.
Now that we have amassed more than 30 years of experience with multifocal IOLs, lens designs have not only become more sophisticated but are also no longer all rotationally symmetric. For instance, the LENTIS Mplus line of IOLs (Mplus and MplusX, both by Oculentis) is built on a rotationally asymmetric, segmental refractive platform design. Both lenses have an aspherical posterior surface and a sector-shaped anterior surface with a near vision add of 3.00 D.
I recently studied the MplusX to determine the lens’ performance in terms of subjective quality of vision, optical phenomena, and spectacle independence at 3 months postoperative. In this article, I briefly discuss the study’s results and outline one case of asthenopia that was resolved by simply rotating the lens postoperatively.
BACKGROUND
In this specific prospective study, 25 patients with bilateral cataract were enrolled. Visual acuity (VA) and contrast sensitivity results are depicted in Figures 1 and 2, respectively. In short, the MplusX provided good binocular distance, intermediate, and near VA, with no patient requiring spectacle correction at 3 months postoperative. Further, patients were generally satisfied after implantation of the LENTIS MplusX, especially during the daytime.1
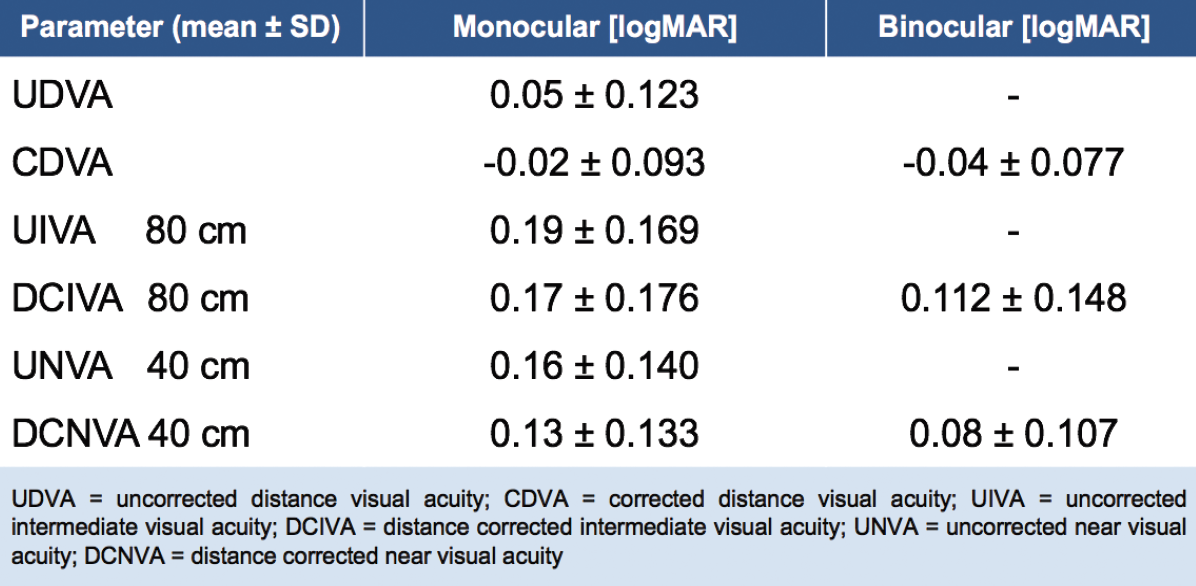
Figure 1. Visual acuity at 3 months postoperative (n = 50 eyes).
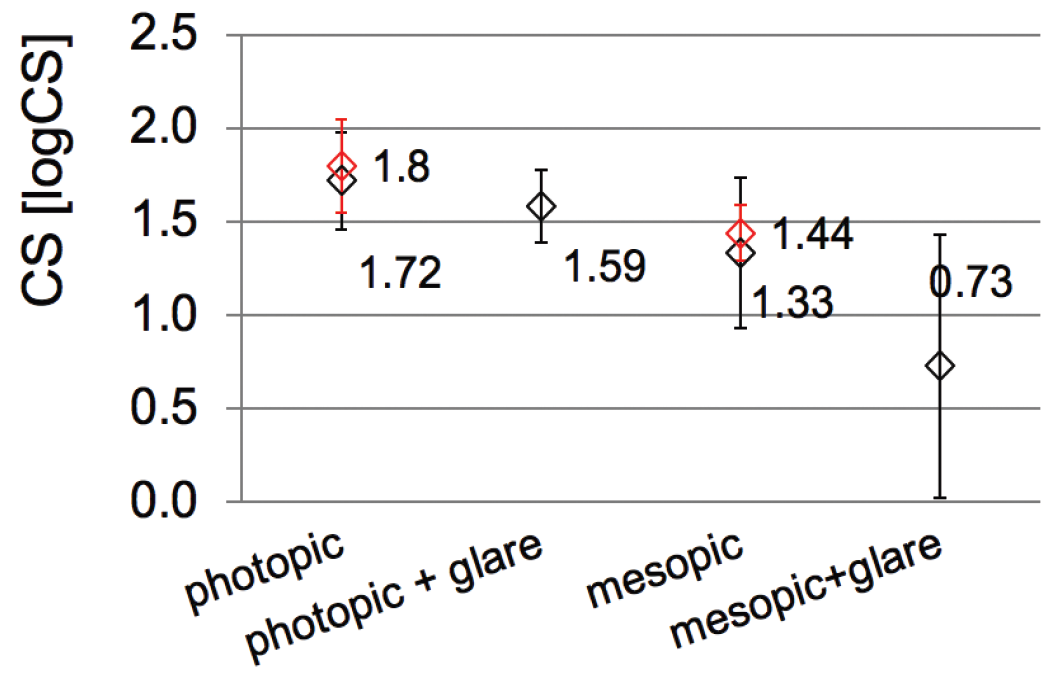
Figure 2. Contrast sensitivity at 3 months postoperative (n = 50 eyes).
At 6 months postoperative, however, one patient returned complaining of symptoms associated with asthenopia, including tired eyes, blurred or double vision, sensitivity to light and glare, headaches, and vertigo. This 76-year-old woman presented postoperatively with corneal edema and a slight increase in IOP during the first few weeks after surgery. Now, she explained that she had the “feeling of wearing the wrong glasses,” and complained that “reading is exhausting.” Her uncorrected and corrected distance visual acuity (UDVA/CDVA) was 0.5/0.8 with +1.25 -0.5 x 100° for OD and 0.8/1.25 with +0.50 -0.25 95° for OS. Anterior and posterior eye exams showed no abnormalities.
COURSE OF ACTION
I decided to check the lens’ stability in the capsular bag to see if perhaps an IOL rotation had occurred, causing these symptoms. Sure enough, in the patient’s right eye, the lens had rotated significantly, causing the near segment to dislocate nasally (Figure 4).
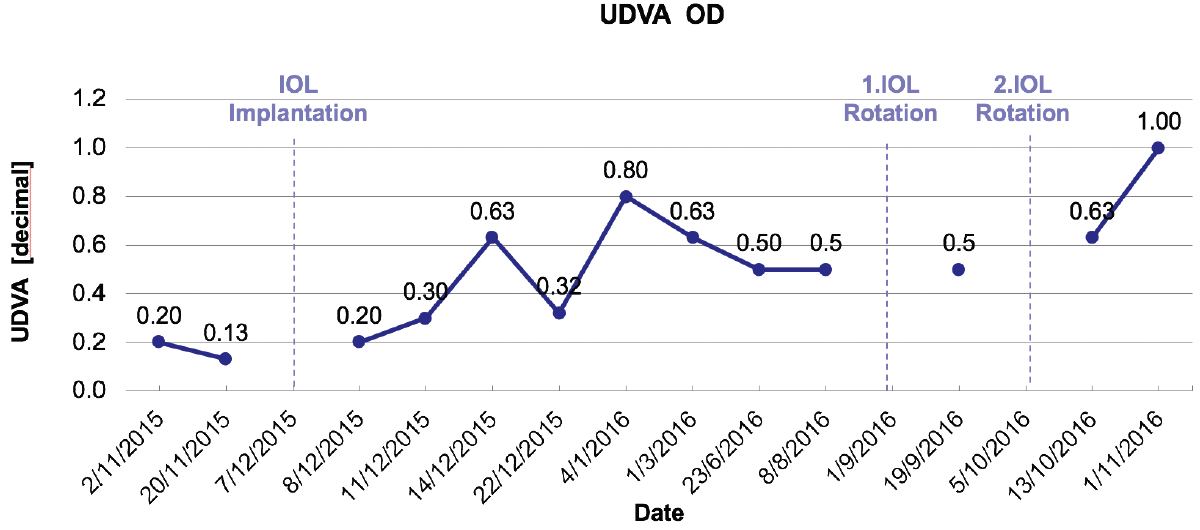
Figure 3. Visual acuity progress.
I scheduled time to return to the OR and re-rotate the lens into its base position, so that the near vision segment was located inferiorly. At the first follow-up examination after the lens was rotated, the patient reported a noticeable improvement in her vision and a decrease in her asthenopic symptoms. Visual improvement only lasted a few days, however, and by 2 weeks, her distance UDVA/CDVA was 0.5/1.0 with a refraction of +1.25 -0.50 x 105º OD. Upon checking the position of the IOL, I noticed the near vision segment had again rotated nasally (Figure 5). I scheduled another intervention to rotate the lens, placing the near vision segment temporally. After this time, the patient’s UDVA improved significantly. Progress of VA results can be found in Figure 3.
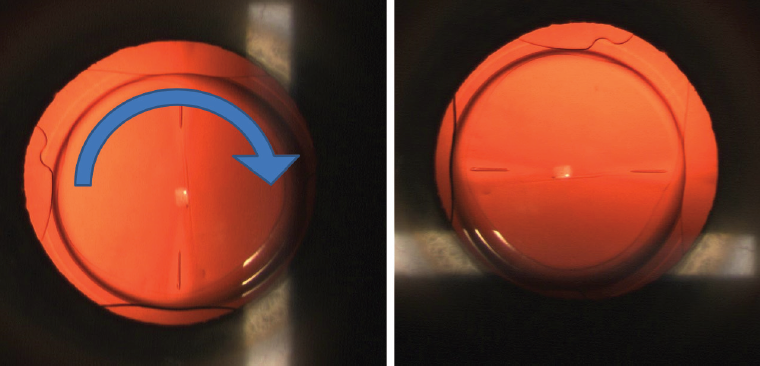
Figure 4. The lens had rotated, causing the near segment to become dislocated nasally.
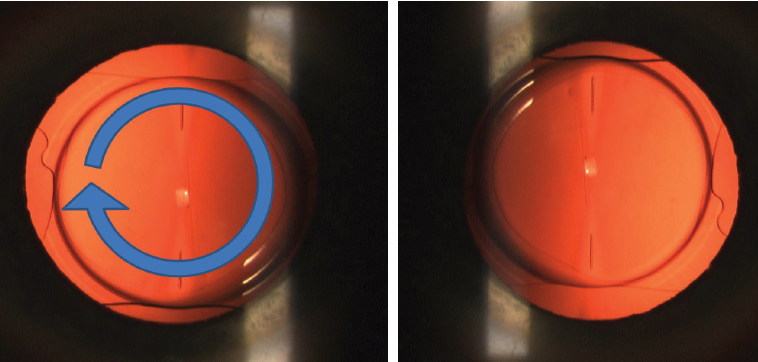
Figure 5. Professor Kohnen rotated the lens a second time, so the near vision is now located temporally.
Although it took nearly 1 year for the patient to achieve the results she had hoped for and the asthenopia to completely resolve, in the end the patient was very happy with her vision and with the MplusX IOL. This case highlights the possibility to rotate the MplusX IOL postoperatively to achieve the desired outcomes and the importance of a thorough postoperative follow-up plan.
CONCLUSION
The MplusX is easily positioned within the eye; however, in the rare case that it rotates postoperatively, positive results can still result. The key is careful placement of the near segment at the manufacturer’s recommended location. When this is achieved, the MplusX is a very useful IOL to meet the high visual demands that our patients have today for every distance.
1. Kohnen T, Hemkeppler E, Herzog M, et al. Visual outcomes after implantation of a segmental refractive multifocal intraocular lens following cataract surgery. Am J Ophthalmol. 2018;191:156-165.
