
Sponsored by Carl Zeiss


Prof. Dr. Bozkurt Sener and Dr. Otto Wolter, COS,
International Vision Centers
Case History
A 36-year-old male presented for refractive error correction. Refraction in his right eye was S: -0.75 D C:-1.25 D Ax: 90. His left eye was S:-1.50 D C: -1.00 D Ax: 80°. Preoperative analyses, including corneal radius of curvature testing, keratometry (Figure 1), and pachymetry, were all unremarkable. Considering the patient’s age, diopter values, corneal quality and the fact that the cylinder axis for both eyes were vertical, my colleagues and I considered him to be a perfect candidate for SMILE. Given his corneal thickness of 540/534 and scotopic pupil of 7 mm, there was no reason not to perform SMILE over a flap procedure, such as PRK or LASIK.
SMILE Treatment
On January 13, 2017 we performed the SMILE surgery. We treated the right eye first. Using the VisuMax Femtosecond System (ZEISS), a refractive lenticule and small incision of 3 mm were created inside the intact cornea– all in one step. The lenticule was subsequently removed through this small incision, leaving the remainder of the superficial cornea intact. Removing the lenticule changed the shape of the cornea, thereby achieving the desired plano refractive correction. The procedure was completed successfully in the right eye without any complications.
Upon starting the procedure on the left eye, we discovered black spots occurring during the first lenticule cut (bottom part of the lower lenticule). We aborted the lenticule formation at the nasal superior location. There was no identifiable reason why the dark spots occurred; however, we cleaned the corneal surface and began the SMILE procedure again. The second effort to create the refractive lenticule and 3 mm incision was completed successfully. However, when we began the manual dissection of the lenticule, the dissection was not possible. After 15 minutes, the lenticule disappeared and became invisible through the microscope due to an occurring edema in the cornea caused by the manual dissection attempts. As a result, dissection and extraction were not possible. We quickly realized that there was no way to remove the lenticule, stopped the process, and decided to postpone the remainder of the procedure until the edema subsided.
My colleagues and I openly and honestly discussed our findings with the patient. We explained that we would remove the lenticule a few days later – after edema would have ebbed away. The patient was happy that we offered an immediate solution. His vision was very good in his right eye and he seemed quite relaxed and unworried about the circumstances surrounding his left eye. He was sent home without any special treatment.
The patient returned the next day for his 1-day postoperative examination and we found that his uncorrected vision was 0.9 D in his right eye and 0.3 D in his left eye. He complained of some discomfort in his left eye due to the large superficial erosion caused by the manual dissection attempts. There were no signs of inflammation, and the edema was declining. We bandaged the left eye and prescribed Trafloxal [Bausch & Lomb/Dr. Gerhard Mann, Germany] for hourly use. We asked the patient to return on the second postoperative day for observation. Upon return, he was experiencing much less discomfort and the erosion had healed. We applied the contact lens bandage for one more day and continued the Trafloxal treatment for one more day.
Since the lenticule was not dissected and removed, we expected UDVA for the left eye to have the same preoperative measurements on day one. While UDVA for the right eye increased to 1.0, surprisingly, UDVA in the left eye also increased from 0.3 to 0.5. Corneal topography showed what we already assumed; the lenticule had been freed completely during manual dissection and moved out of the center optical zone (Figure 2). It was now folded up outside the optical zone. It was clear that the patient’s vision improved day by day as the edema declined. On the third postoperative day, UDVA in the left eye had increased from 0.5 to 0.7. The right eye remained stable at 1.0. Since the edema had disappeared completely, we asked the patient to return at the 1-week postoperative visit to remove the lenticule. Due to the patient’s availability, the surgery was postponed to 1 month after the initial surgery. Because his UDVA was 0.7 in the left eye and 1.0 in the right eye, there was no need to correct his vision for the remaining weeks before the lenticule was to be removed.
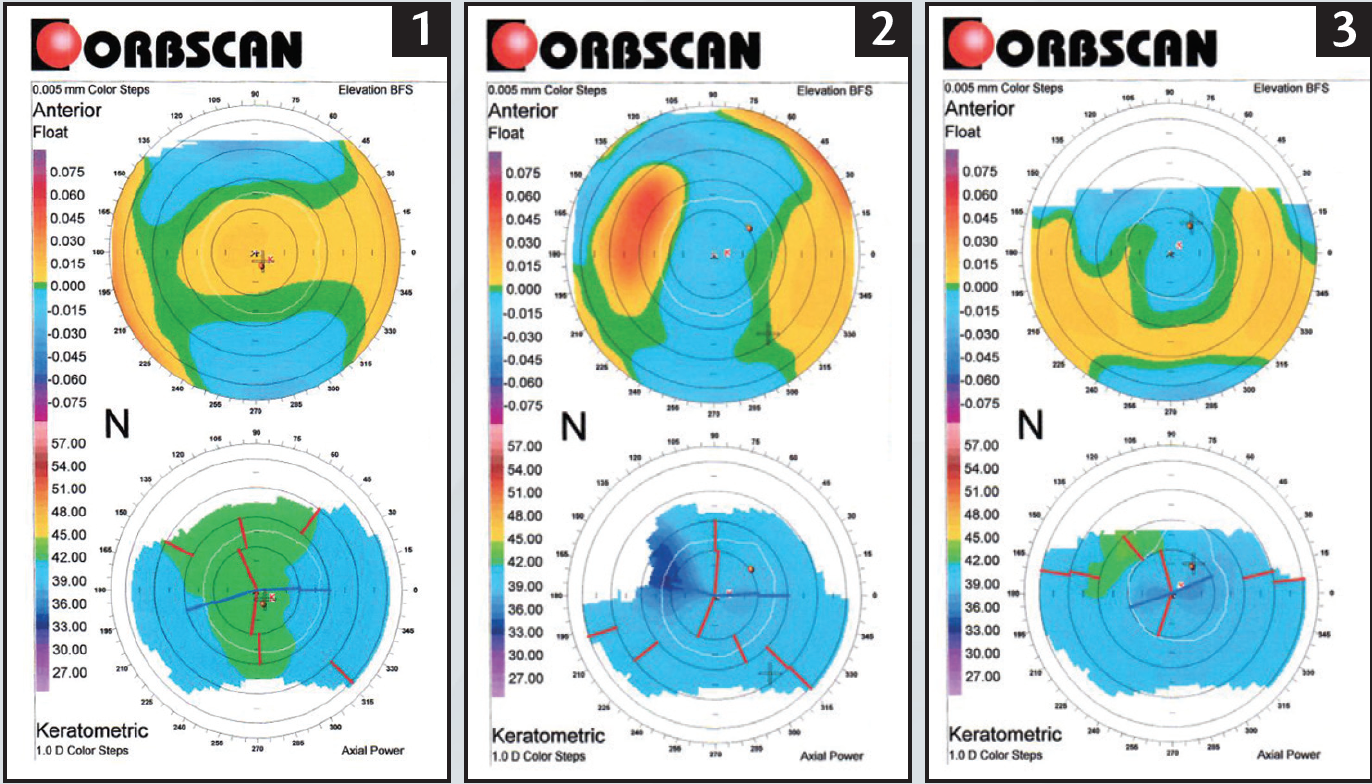
Figure 1-3: Anterior Elevation (BFS) and Axial Power pre-op (1), after SMILE surgery but lenticule was not extracted yet (2), after lenticule extraction (3).
SECOND TREATMENT
When the patient returned on February 7 2017, his edema had gone completely. We performed a slit-lamp examination and obtained corneal topography imaging. As we indicated on the second postoperative day, the lenticule could easily be located in the nasal area under the cap via the slit-lamp examination. The patient’s vision in his left eye had improved further from 0.7 to 0.8, and theright eye was stable with 1.0 UDVA.
The same surgeon who performed the initial procedure was able to easily remove the lenticule within 30 seconds and in one piece with forceps. On postoperative day one, the right eye was still 1.0 and the left eye had improved to 0.9 UDVA (Figure 3).
CONCLUSION
When refractive surgeons are facing difficulties during the lenticule separation or extraction of SMILE, stay calm and keep cool. There is no reason to be shocked, worried, or angered by pressure to extract the lenticule immediately. The possible expected complications after the incomplete SMILE procedure, such as remaining poor vision, inflammation, dramatic loss of visual acuity, remaining cylinder, or extreme discomfort for the patient did not occur. This experience proves that it is better to interrupt the surgery and wait until difficulties are resolved, in this case edema, and postpone the procedure for a later date. If it is necessary to postpone the procedure, monitor the patient with follow-up visits until the procedure can be completed and support the patient to alleviate any feelings of discomfort. Finally, talking to patients in an honest and open way keeps them informed and comforted during the transition and enhances the treatment experience. In the end, patients will still be highly satisfied as the surgeon will still be able to get them close to their target refraction with SMILE with a stable refractive correction.