
For many years now, the EVO Visian ICL (previously known as the Visian ICL V4c; STAAR Surgical) has been my elective procedure of choice for young patients between the ages of 21 and 45 years who desire refractive correction for -0.50 to -18.00 D myopia and, with the toric version of the lens, up to 6.00 D astigmatism. In my patients, I have consistently seen excellent postoperative outcomes, with high patient satisfaction and little to no visual disturbances. When visual disturbances had been noted by patients, in many cases, it was due to their large pupil size, which caused them to experience a diffraction effect that most commonly presented as halos.
Now, variations of the EVO with an expanded optic, the EVO+ and EVO+ Toric, are available to better accommodate the ocular anatomy of patients with larger pupils. This increase in the lens’ surface (up to 20% depending on the lens power), creates more pupil coverage, and may improve meso-scotopic vision quality, and, therefore, likely results in a decrease of the diffraction effect.
The only difference between the EVO and EVO+ lenses is, indeed, the expanded optic of up to 6.1 mm in optic zone diameter. Both are made with the company’s proprietary advanced collamer lens material, which is biocompatible with the eye, UV-A protectant, and soft and pliable to promote easy implantation. As a result, there is no need to modify one’s surgical technique or power calculation and sizing methods when implanting the EVO+.
PERSONAL EXPERIENCE
Since 2011, I have been implanting models of the ICL that incorporate the KS-Aquaport*, a hole in the center of the lens that eliminates the need for an iridectomy or iridotomies. In the past 6 years, I have implanted more than 700 ICLs. Most recently, in February 2016, I implanted the very first EVO+ Visian ICL. Thus far, results with this lens have been just as good as they were with the EVO Visian ICL, and refractive accuracy and visual quality of the lens have been impressive. My experience is not unique; in their study, Domínguez-Vincent et al1 found that the optical quality of the EVO+ was comparable not only to the EVO but also to the natural crystalline lens. They also found no significant differences in higher-order aberrations between the lenses, including total root mean square, coma, trefoil, tetrafoil, and secondary astigmatism in any power and aperture. They had analyzed lens models in four powers over 3- and 6-mm pupil sizes.
I recently conducted a study of 50 eyes of 27 patients who received the EVO+ Visian ICL or EVO+ Visian ICL Toric at my practice between February 23 and August 23, 2016. A lens with an overall size of 12.6 mm was implanted in 12% of eyes, of 13.2 mm in 80%, and of 13.7 mm in 8%, and the mean spherical equivalent was -8.89 ±2.36 D (range, -5,00 to -14.00 D). The toric ICL was indicated if the eye presented with at least 1.25 D astigmatism.
In all cases, the lens was implanted via a 2.75-mm incision on the steep axis. I used an OVD with a low molecular weight and viscosity, as recommended by STAAR Surgical. Postoperative follow-up including refraction, biomicroscopy, IOP, and vault was scheduled for 1 day and 1 and 4 weeks after surgery.
RESULTS
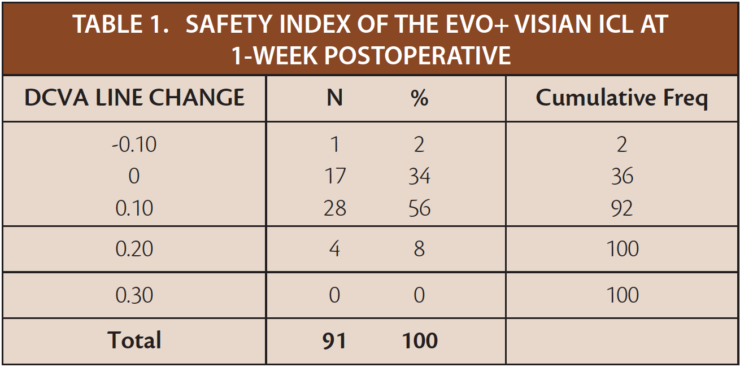
Efficacy. At 1-week postoperative, 100% of eyes were within ±0.50 D of intended correction (Figure 1). As means of comparison, in a sampling of eyes that received the EVO Visian ICL in 2013, 98.9% were within ±1.00 D of intended correction, and 90.11% were within ±0.50 D. The EVO+ lens also boasted excellent BCVA at 1-week and 1-month postoperative (Figure 2), with a safety index of 1.12 at 1-week postoperative (Table 1). In the same sampling of EVO eyes from 2013, the safety index at 6 months postoperative was 1.20.
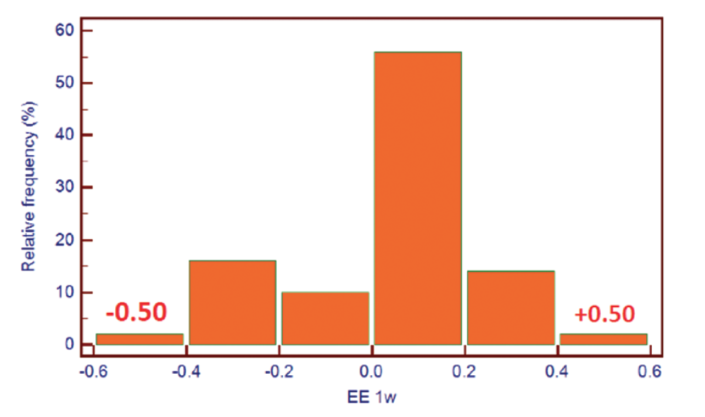
Figure 1. Efficacy at 1 week postoperative: 100% of eyes were within ±0.50 D spherical equivalent.
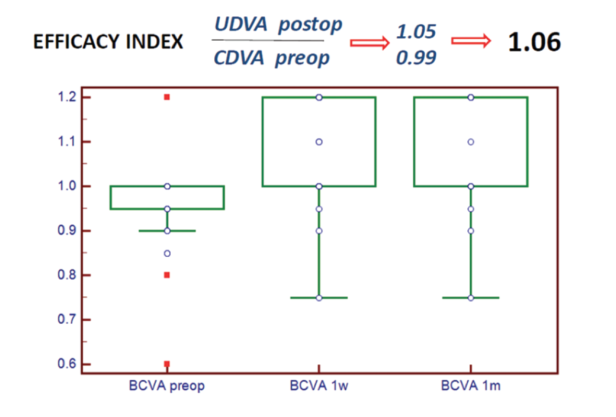
Figure 2. BCVA at 1 week and 1 month postoperative.
IOP. When we looked at mean IOP, at 1-week postoperative, it was slightly higher than it was preoperatively (18.48 vs 16.62 mm Hg, respectively). However, by the 1-month follow-up, the mean IOP had returned to preoperative levels (16.65 vs 16.62, respectively).
Vault. The mean vault at 1-month postoperative was 611.38 ±182.07 μm, which was slightly better than the mean vault that we had been able to achieve with the standard EVO Visian ICL. In the majority of eyes that received the EVO+ (92.5%), the vault was between 300 and 1,000 μm. In one eye with a low vault (280 μm), the lens had been implanted vertically. Once rotated to the horizontal meridian, the vault increased to 680 μm. In another case, a high vault of 1,160 μm was found, and the lens was rotated at a later time to the horizontal meridian. The final vault in that case was 740 μm.
Patient satisfaction. On a scale of 0 to 5 (0 = very good, 5 = very bad), patients who received the EVO+ Visian ICL were asked to rate their visual quality with regards to the presence of halos and ghost images and the impact they have had on visual function and life tasks. Scores were then compared to those reported by patients who had previously received the EVO model (Figure 3). Like the EVO, patients with the EVO+ seemed to experience halos early postoperatively but reported that they improved over time. By 1-month postoperative, all patients were happy with their visual outcomes.
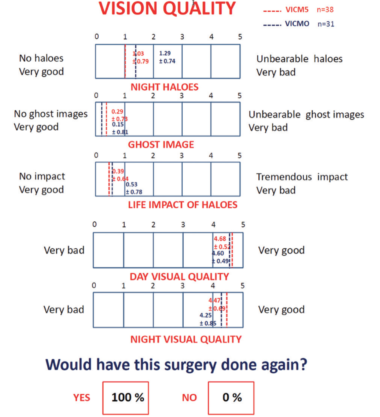
Figure 3. Patient satisfaction survey: vision quality.
In three patients included in the study of the EVO+, an EVO lens had previously been implanted in the contralateral eye. One of these patients, who was emmetropic in both eyes and had a 6.5-mm scotopic pupil, reported better mesopic visual quality in the eye that received the EVO+. The other two patients reported no differences in visual quality or in overall satisfaction between their eyes.
CONCLUSION
I have reported no significant difference in the folding, cartridge loading, unfolding, and footplate manipulation between the EVO+ and EVO Visian ICLs. Likewise, there has been no difference with the vault and refractive precision of the lenses. What I have noticed, however, is an improvement in visual quality due to the EVO+’s wider optical zone decreasing the diffraction effect. At present, I only implant the EVO+ Visian ICL in patients who present with -14.00 D myopia or less.