
There is no doubt that we refractive surgeons are masters of our trade. We stay abreast of the latest advancements and the newest procedures, and we vow to offer patients what we believe are the best and most effective treatments to obtain the refractive outcomes they desire. Sometimes, however, we must take a step back from this and ask ourselves if a given treatment or trend measures up not only clinically but also financially.
In the same vein, recently, my colleagues and I worked with a consultant to conduct a profitability analysis of our Smile Eyes center in Munich, Germany. Of the 11 Smile Eyes centers across Germany and Austria, this is our busiest, as approximately 1,200 refractive procedures are performed here annually. Among the total number of refractive procedures, small incision lenticule extraction (SMILE) and femtosecond LASIK account for 70% of our volume. These procedures are preferred in patients with refractive errors between 3.00 and -8.00 D. The other 30% of our total refractive surgery volume is made up of refractive lens exchange (20%) and phakic IOL implantation (10%). These procedures are preferred in patients with high hyperopia and high myopia and in patients with irregular corneas. Looking at only phakic lens implantation procedures, in some cases we implant the lens as a standalone procedure and in others in combination with a laser treatment, in what is referred to as a bioptics procedure.
One of the main reasons that we initially offered bioptics to our patients was because the AcrySof Cachet (Alcon), the phakic IOL that we had been previously using for years, was not available in a toric version. Even after we switched to the Visian ICL (now EVO Visian ICL; STAAR Surgical), a phakic IOL that is available in a toric version, we had continued to offer bioptics as an option for our patients. The reason for this was that we first wanted to gather some clinical experience with the toric ICL. After we found out that this lens was stable and that results were excellent, we only offered bioptics to patients as a more cost-effective solution due to the higher price of the toric implant.
But was it still financially worthwhile for our practice to continue offering this package? This is what we set out to discover through the profitability analysis. One thing to point out, however, is that we did not want to modify in any way our indications for surgery; we wanted to continue treating refractive errors between 3.00 and -8.00 D with a laser-based procedure and high hyperopia and high myopia and patients with irregular corneas with a lens-based procedure.
ANALYSIS
Conducting the profitability analysis required us to look at several things: our pricing strategy, our operational process scheme, and the types of costs associated with our process.
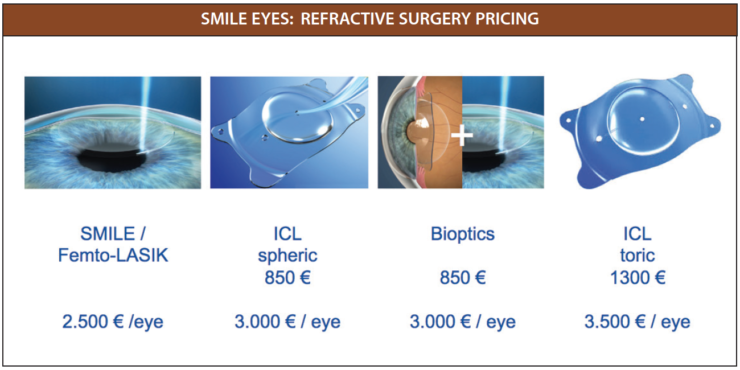
Pricing strategy. First, we broke down our pricing strategy per eye (see Smile Eyes: Refractive Surgery Pricing). When we originally devised our price points, we placed a logical gap between pricing for the spherical EVO Visian ICL and bioptics procedures (both at €3,000/eye) and pricing for the EVO Visian ICL Toric procedure (€3,500/eye). This was purely due to the higher cost of the toric version of the lens. It did not take into account any additional costs, such as personnel or equipment.
Simplified process scheme. We then outlined our simplified process scheme, which included marketing, patient consultations, the surgery itself, postoperative follow-up and care, and invoicing (Figure 1).
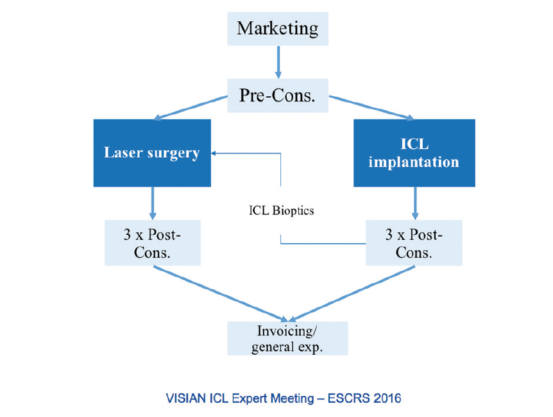
Figure 1. A simple outline of the process scheme used by Smile Eyes.
Types of costs. The third and most time-consuming part of the profitability analysis was to determine the various costs associated with each procedure. We broke this down into four components: personnel costs, including the surgeon, anesthesiologist, ophthalmologist, theatre nurse, and technician; occupancy costs, including the operating room, consultation, and rent and incidental rent expenses; equipment costs, including the purchase depreciation and maintenance costs for the following equipment: femtosecond laser, excimer laser, microscope, and phacoemulsification machine; and material costs, including the EVO Visian ICL, expendable materials, and treatment packs.
Once we broke down the personnel cost per minute (Table 1), we were then able to compare the amount of money we spent per lens-based procedure (EVO Visian ICL, bioptics, and EVO Visian ICL Toric) across all components. Whereas we spent roughly the same amount of money on marketing, administration, and occupancy for all three procedures, the personnel and equipment costs were highest with the bioptics procedure, and the material costs were highest in the EVO Visian ICL Toric procedure (Figure 2). When we looked at the total costs and profit associated with each procedure, we found that the bioptics procedure cost us the most and produced the smallest profit margin (Figure 3). The profit margins for both of the EVO Visian ICL procedures were similar.
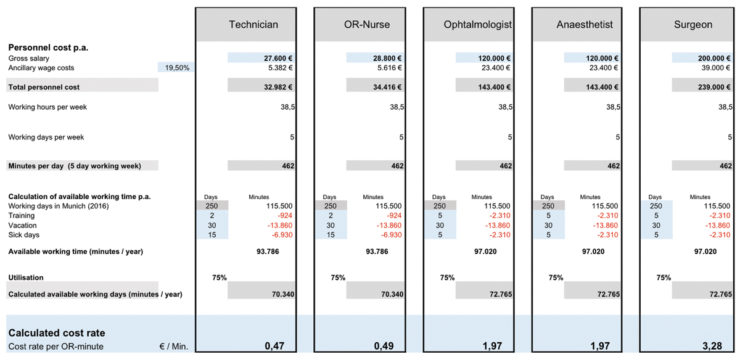
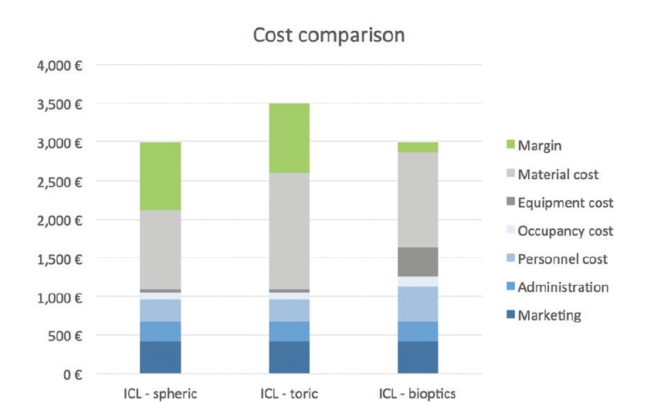
Figure 2. Cost comparison of three refractive surgery procedures: EVO Visian ICL, EVO Visian ICL Toric, and bioptics (combination ICL/laser vision correction).
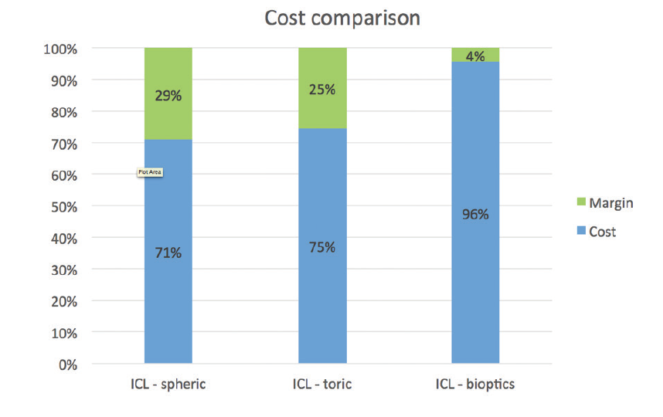
Figure 3. Profitability margins for the three procedures.
LESS OF A PROFIT
Through our profitability analysis, we discovered that we were making only €150/eye with the bioptics procedure. Although still a profit, it was significantly less of a profit than we were making with both ICL procedures. We were quite surprised by that, and, in the end, we decided against continuing to offer patients the option of a bioptics procedure.
Although the profitability analysis is unique to our clinic—because of our own pricing strategy and our own personnel, occupancy, equipment, and material costs—the overall message that can be extrapolated is this: offering the EVO Visian ICL Toric instead of bioptics can be a more profitable strategy.
CONCLUSION
The bottom line continues to be that just like any other refractive surgery practice, we do what is best for the patient. That, for us, is the EVO Visian ICL and EVO Visian ICL Toric. With this strategy, we can offer patients correction of their refractive error in a single treatment, which makes more sense not only for the patient but financially for our practice as well.
