
Sponsored by STAAR Surgical

I have, for many years now, relied on a multitude of therapies for the management of keratoconus. These therapies, which range from therapeutic approaches like intrastromal corneal ring segment (ICRS) implantation, CXL, and keratoplasty to refractive approaches like PRK, lensectomy, and phakic IOLs. In some cases, I have even combined treatments, of which the most common is ICRSs with a phakic IOL.
Most recently, I have studied the use of ICRSs with the Visian ICL Toric (now EVO Visian ICL Toric; STAAR Surgical), to address the needs of patients with stable keratoconus (grades 1–3). A similar treatment was first described by Coskunseven et al1 in 2007. In that study, two patients with keratoconus and extreme myopia first received Intacs (Addition Technology), followed 6 to 10 months later with the Visian ICL Toric. Alternatively, in my procedure, I first implant the Keraring (Mediphacos), followed sequentially with implantation of the EVO Visian ICL 6 months later. To date, I have seen successful results with this approach in patients across the range of keratoconus phenotypes outlined in Classification of Keratoconus. This classification system is further explained in a doctoral thesis by Fernández-Vega Cueto.2

RETROSPECTIVE STUDY
In order to assess the visual and refractive results of the combination of ICRSs with the EVO Visian ICL for the treatment of stable keratoconus, I conducted an observational, longitudinal, retrospective study of 42 eyes of 30 patients.3 The mean age of this population was 34.8 ±6 years (range, 21–43 years). All patients had keratoconus with coincident topographic and comatic axes, flattest keratometry (K) between 40.00 and 50.00 D, keratometric astigmatism lower than 9.00 D, and significant myopia or hyperopia. Preoperatively, the mean UDVA was 0.1 ±0.1 (range, 0.1–0.3); the mean CDVA was 0.6 ±0.2 (range, 0.2–0.9); the mean sphere was -8.00 ±6.60 D (range, -17.25 to 3.25 D); and the mean refractive cylinder was -3.82 ±1.90 D (range, -7.00 to -1.00 D).
In all cases, the patient first received the 5-mm Keraring model, and a corneal thickness implantation zone of at least 400 μm was respected. With this treatment modality, the mean UDVA, CDVA, sphere, and refractive cylinder improved to 0.2 ±0.2 (range, 0.1–0.7), 0.8 ±0.2 (range, 0.4–1.0), -6.26 ±6.90 D (range, -20.00 to 3.50 D), and -1.99 ±1.10 D (range, -4.00 to 0.00 D), respectively.
Then, 6 months after Keraring implantation, all patients received the EVO Visian ICL. During this second procedure, one or two 3.2-mm opposite clear corneal incisions (CCIs) were also created, in order to address the keratometric astigmatism. After this treatment, the mean UDVA, CDVA, sphere, and refractive cylinder once again improved, to 0.6 ±0.2 (range, 0.2–1.0), 0.8 ±0.1 (range, 0.5–1.0), -0.21 ±0.70 D (range, -2.00 to 1.50 D), and -0.88 ±0.70 D (range, -2.00 to 0.00 D), respectively.
Regarding safety of the combined procedure, 73% of patients gained 1 to 3 lines of BCVA, whereas 15.79% neither gained nor lost and only 10.53% lost 1 line of BCVA (Figure 1). As a comparison, 68% of patients had gained 1 to 3 lines of BCVA after the initial ICRS treatment, 15.79% remained unchanged, and 15.79% lost 1 line (Figure 2). What is especially interesting is that the percentage of patients who gained 2 or more lines increased from 5.26% after the ICRS treatment to 26.32% after the EVO Visian ICL was implanted.
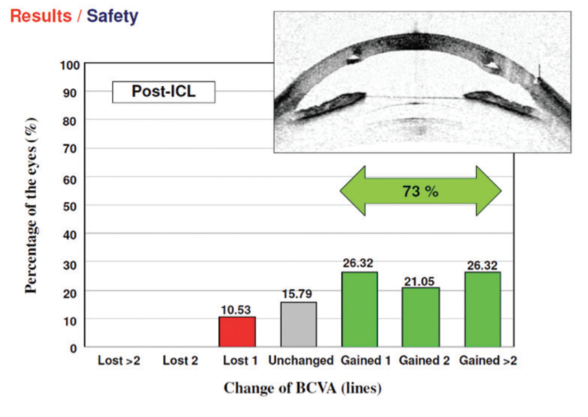
Figure 1. Changes in BCVA after EVO Visian ICL implantation.
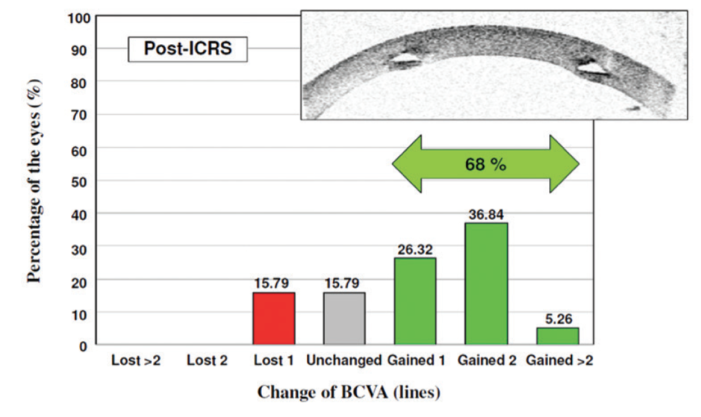
Figure 2. Changes in BCVA after ICRS implantation only.
The refractive predictability in both cylinder and sphere corrections was good, with 78% of patients within ±1.00 D of intended correction for sphere and 61% for cylinder after ICL implantation combined with CCI creation.
A SECOND COMBINATION: ICRSs, ICL TORIC
Given our excellent outcomes with the combination of ICRSs, EVO Visian ICL, and opposite CCIs in patients with stable keratoconus, and given the excellent results with the EVO Visian ICL Toric both in a standalone procedure4 and in combination with CXL,5 we recently decided to also try combining ICRSs with the EVO Visian ICL Toric. We performed our first cases in 2016, of which one is described herein.
A 30-year-old man with stable keratoconus, steep K of 50.00 D, and refraction -6.00 -6.00 X 150º presented for surgery. His UDVA and CDVA were 0.16 and 0.6, respectively. After we implanted a 210º Keraring, he had a refraction of -5.00 -4.00 X 125º, with UDVA and CDVA of 0.3 and 0.7, respectively.
Six months later, we implanted a EVO Visian ICL Toric lens with powers of -10.50 D sphere and 5.50 D cylinder (Figure 3). Once again mean UDVA, CDVA, sphere, and refractive cylinder improved postoperatively, to 0.6, 0.8, -1.00 D, respectively.
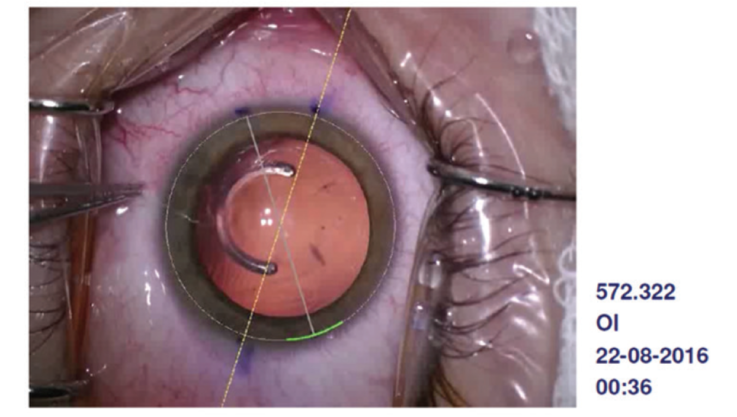
Figure 3. In this case, the 210º ICRS was placed at 90º, followed by the implantation of the EVO Visian ICL Toric.
Although no long-term follow-up is available and the procedure has only been performed on a small number of patients to date, our preliminary results are encouraging. I look forward to presenting more results on this combination in more patients in the near future.
CONCLUSION
With many therapies available for the treatment of keratoconus, it can be hard for surgeons to pinpoint what strategy is best. In my experience, the combination of ICRSs and the EVO Visian ICL spherical and toric lenses is an effective and safe procedure in patients with stable keratoconus. The ICRS can be used to target corneal irregular astigmatism, and the ICL can be used to target the residual sphere and corneal astigmatism.
I urge surgeons who are considering this strategy to keep at least 6 months in between the sequential treatments.
1. Coskunseven E, Onder M, Kymionis GD, et al. Combined Intacs and posterior chamber toric implantable collamer lens implantation for keratoconic patients with extreme myopia. Am J Ophthalmol. 2007;144:387-389.
2. Fernández-Vega Cueto, “Classification of Keratoconus for its surgical correction with Ferrara-type ICRS” PhD diss.
3. Alfonso JF, Lisa C, Fernández-Vega F, et al. Intrastromal corneal ring segments and posterior chamber phakic intraocular lens implantation for keratoconus correction. J Cataract Refract Surg. 2011;37:706-713.
4. Kamiya K, Shimizu K, Kobashi H, et al. Three-year follow-up of posterior chamber toric phakic intraocular lens implantation for the correction of high myopic astigmatism in eyes with keratoconus. Br J Ophthalmol. 2015.
5. Antonio R, Dirani A, Fadlallah A, et al. Safety and visual outcomes of Visian Toric ICL implantation after corneal collagen cross-linking in keratoconus: Up to 2 years of follow-up. J Ophthalmol. 2015.
