
Implantation of phakic IOLs has been an accepted practice to correct refractive errors since the introduction of angle-supported phakic IOLs in the 1950s. The practice had continued through the 1980s with iris-fixed lens models and the 1990s with posterior chamber designs such as the Implantable Collamer Lens (now Visian ICL; STAAR Surgical).1-6 In 2015, phakic IOLs still present good refractive surgical options for anterior segment surgeons. The implantation of phakic IOLs remains an acceptable solution, particularly for patients who are not suitable for laser refractive surgery or refractive lens exchange.
Phakic IOLs have not been without controversy, particularly because of their possible side effects and complications including endothelial cell loss and cataractogenesis. In recent years, optimization of lens designs and of inclusion criteria have led to minimization of these phenomena. When cataract does occur after phakic IOL implantation—no matter whether its formation was a consequence of the IOL implantation or physiologic processes—the anterior segment surgeon is asked to provide a solution. Although explantation of these lenses and subsequent cataract extraction is not a great challenge for an experienced surgeon, there are additional options in the era of laser-assisted cataract surgery (LACS). We present such a case in this article.
PRESENTATION AND HISTORY
A 32-year-old woman with phakic IOL implants presented at our clinic with the chief complaint of an increasing loss of visual acuity and glare, especially at night. The phakic IOL implantation was performed bilaterally 9 years previous in our clinic with implantation of two Visian ICLs (Model ICM115V4). Refraction at the time of ICL implantation was -8.50 -0.75 X 80° OD and -8.50 -0.25 X 75° OS. There was no contraindication for phakic IOL implantation. The operations were performed under general anesthesia without complication. One month postoperatively, refraction was +0.25 -0.75 X 3° OD and 0.00 -0.75 X 164° OS. Distance UCVA was 20/16 OD and 20/16 OS.
AT A GLANCE
• Manipulating or explanting an ICL requires care with
the laser-created capsulorrhexis to avoid tears or
runouts in case the rhexis is incomplete with capsular
adhesions.
• LACS can be performed after previous implantation of
a variety of phakic IOL models; however, there may be
some risk when the procedure is applied in phakic eyes
with iris-fixated IOLs.
Annual monitoring of endothelial cell count and the anterior segment was performed, and the patient enjoyed the benefits of a life without glasses or contact lenses. Then the patient presented 9 years postoperatively with the symptoms described above. Her distance UCVA was significantly reduced at 20/40 OD and 20/63 OD. Autorefraction values were -0.50 -0.75 X 18° OD and -1.25 -0.75 X 169° OS. Subcapsular cataracts were seen in each eye, especially OD.
Because of the young age of the patient and her BCVA of 20/16, we performed bilateral myopic PRK. This resulted in distance UCVAs of 20/16 OD and 20/16 OS. After the elapse of another 3 years, the patient complained again of a reduction in visual acuity OD only; examination showed progression of the subcapsular cataract. Refraction in this eye was +1.25 -0.75° X 128º, distance UCVA was 20/32, and distance BCVA was 20/25.
After extensive discussion with the patient, we decided to perform LACS in her right eye without prior manipulation of the phakic IOL. Because of her desire not to wear eyeglasses and in the absence of contraindications, we decided to implant a trifocal IOL. The IOL calculation was performed with the IOLMaster (Carl Zeiss Meditec) using the Haigis L formula for eyes after myopic LASIK.
STEPS IN THE TREATMENT PLAN
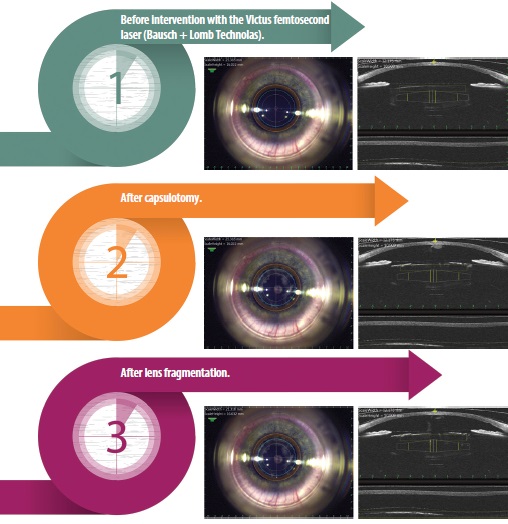
SURGERY AND POSTOP COURSE
A 5.3-mm overlapped capsulorrhexis was created, and lens fragmentation with two circular and four radial cuts was performed with the femtosecond laser. The energy was set to 7,000 nJ (see Steps in the Treatment Plan). The lens fragmentation through the ICL was performed without complications. Subsequently, the ICL was explanted as usual through a 3.5-mm tunnel, and implantation of an AT LISA trifocal IOL (Carl Zeiss Meditec) was performed. Because the UCVA OS was 20/16, no intervention was performed in this eye.
The 1-month examination showed perfect centration of the IOL and an individually adapted capsulorrhexis. The visual result of distance UCVA 20/20, intermediate UCVA 20/20, and near UCVA 20/20 OD led to a high degree of satisfaction in the patient.
DISCUSSION
As demonstrated in the case presented here, previous implantation of a phakic IOL is no obstacle to take advantage of the femtosecond laser technology. When manipulating or explanting the ICL, care should be taken with the laser-created capsulorrhexis to avoid tears or runouts in case the rhexis is incomplete with capsular adhesions. The accumulation of gas bubbles under the ICL did not lead to any special conditions or difficulties.
The procedure could possibly be applied in eyes with different types of previously implanted phakic IOLs, such as iris-fixated or angle-supported lenses. However, we believe that there is some risk when the procedure is applied in phakic eyes with iris-fixated IOLs: The harder nonelastic material, in combination with the accumulation of air bubbles, might cause trauma to the iris in the location of haptic fixation. There are not many experiential reports published with such cases, so in the future it will be interesting to learn more from other authors about the limits and capabilities of the femtosecond laser for these applications.7,8 n
1. Güell JL, Morral M, Kook D, et al. Phakic intraocular lenses part 1: historical overview, current models, selection criteria, and surgical techniques. J Cataract Refract Surg. 2010;36:1976-1993.
2. Strampelli B. Tolerance of acrylic lenses in the anterior chamber in aphakia and refraction disorders. Ann Ottalmol Clin Oculist. 1954;80:75-82.
3. Barraquer J. Anterior chamber plastic lenses. Results of and conclusions from five years´s experience. Trans Opthalmol Soc UK. 1959;79:393-424.
4. Kohnen T, Kook D, Morral M, et al. Phakic intraocular lenses: part 2: results and complications. J Cataract Refract Surg. 2010;36:2168-2194.
5. Rosen E, Gore C. STAAR Collamer posterior chamber phakic intraocular lens to correct myopia and hyperopia. J Cataract Refract Surg. 1998;24:596-606.
6. Gonvers M, Bornet C, Othenin-Girard P. Implantable contact lens for moderate to high myopia: relationship of vaulting to cataract formation. J Cataract Refract Surg. 2003;29:918-924.
7. Tomalla M, Doulgkeridis I. Presbyopia correction with laser and lens treatments. Cataract & Refractive Surgery Today Europe. October 2013; 62-66.
8. Tomalla M. Femtosecond Laser—Principles and Application in Ophthalmology. Bremen, Germany: Uni-Med Verlag AG/International Medical Publishers; 2010.
Ioannis Doulgkeridis
- Resident physician, Center for Ophthalmology, Clinic for Refractive and Opthalmosurgery, Duisburg, Germany
- joannis.doulgkeridis@evkln.de
- Financial disclosure: None
Mark Tomalla, MD
- Director, Center for Ophthalmology, Clinic for Refractive and Opthalmosurgery, Duisburg, Germany
- mark.tomalla@evkln.de
- Financial disclosure: Consultant (Bausch + Lomb Tecnolas, Carl Zeiss Meditec)
