


Sulcoflex Pseudophakic Supplementary IOLs (Rayner) are my lenses of choice whenever piggybacking of an IOL is required. I have used these IOLs in the following situations:
- To address post–cataract surgery refractive surprise;
- For lens exchange when a three-piece lens placed in the sulcus has become decentered; and
- For pseudophakic emmetropes who realize postoperatively that they desire more intermediate or reading vision. In this situation, a plus-powered lens can be implanted in the sulcus to make the nondominant eye slightly myopic and achieve IOL monovision, mini-monovision, or blended vision.
Although laser eye surgery remains the gold standard and treatment of choice for refractive enhancements, many patients in the pseudophakic age group, especially cataract surgery patients, do not have a good quality ocular surface. This makes laser eye surgery potentially more problematic due to the risk of inducing dry eye syndrome. In these patients, my preference is for an IOL solution rather than laser eye surgery.
AT A GLANCE
• Piggybacking an IOL such as the Sulcoflex is a good option to address post–cataract surgery refractive surprise; for lens exchange when a three-piece lens placed in the sulcus has become decentered; and for pseudophakic emmetropes who realize postoperatively that they desire more intermediate or reading vision.
• The Sulcoflex is designed for sulcus placement, and several features encourage good stability and centration of the lens and prevent iris chafing and pigment dispersion.
VERSATILE PLATFORM
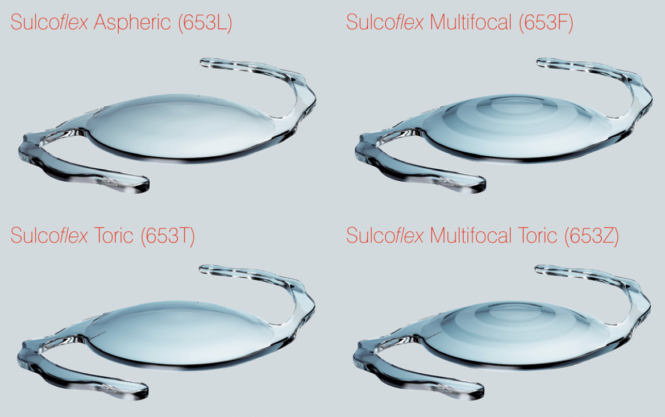
The Sulcoflex range of pseudophakic IOLs includes aspheric, multifocal, toric, and multifocal toric optic configurations (Figure 1). This IOL platform has several advantages over alternative lens options in my experience. The Sulcoflex has been specifically designed and engineered for sulcus placement, and it has several key features that demonstrate this.
Courtesy of Rayner
Figure 1. The Sulcoflex is available in aspheric, multifocal, toric, and multifocal toric models.
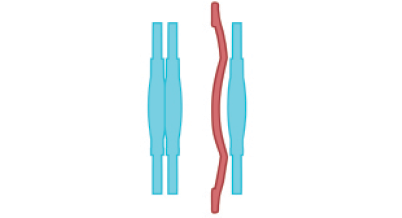
Key Feature No. 1. An increased haptic length and undulated haptic design (Figure 2), which encourages good stability and centration of the lens in the sulcus and prevents iris chafing and pigment dispersion;
Courtesy of Rayner
Figure 2. The increased haptic length and undulated haptic design of the Sulcoflex encourage good stability and centration of the lens in the sulcus and prevent iris chafing and pigment dispersion.
Key Feature No. 2. Angulated haptics to ensure that the IOL sits posteriorly, which prevents iris chafing and pigment dispersion;
Key Feature No. 3. A rounded anterior surface of the optic to prevent iris chafing and pigment dispersion; and
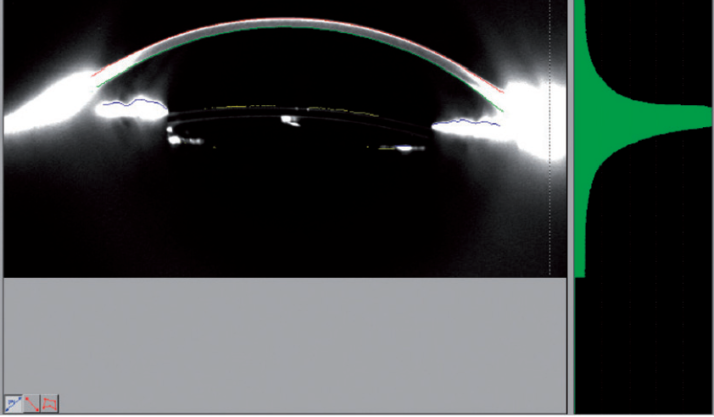
Key Feature No. 4. An anterior-convex optic design to ensure that it does not make contact with the in-the-bag IOL (Figure 3).
Courtesy of Rayner
Figure 3. The posterior concave surface of the supplementary Sulcoflex minimizes the possibility of interaction with the primary IOL.
Rayner offers an online calculator specific to the Sulcoflex (https://www.raytrace.rayner.com). The refractive target can be input, along with other measurements pertinent to the patient’s eye (eg, axial length and anterior chamber depth), and the desired power for the Sulcoflex IOL is then generated.
SULCOFLEX TO THE RESCUE
I have used Sulcoflex lenses many times, but one case in particular comes to mind. An 86-year-old woman with bilateral dense cataracts and with-the-rule corneal astigmatism presented for cataract surgery. Her visual acuity was limited to 20/80 in each eye. She was motivated to be independent of glasses for distance activities but happy to wear glasses for reading, so I targeted emmetropia with a T-Flex Aspheric Toric IOL (Rayner) in each eye.
The Lens: Sulcoflex Pseudophakic Supplementary IOLs
RAYNER
• Available in aspheric, multifocal, toric, and multifocal toric models
-Aspheric allows correction of residual refractive error
−Multifocal incorporates 3.50 D near add at IOL plane (distance-dominant format)
-Toric offers alternative to corneal incisions with a range of cylinder powers
-Multifocal toric incorporates 3.50 D add plus 1.00 to 3.00 D cylinder correction
• Undulating haptics help stabilize IOL to avoid rotation
• Posterior haptic angulation and anteriorly convex optic help avoid iris contact
• Large 14-mm overall length facilitates sulcus placement
• Large 6.5-mm optic with rounded edges designed to reduce risk of iris capture and edge glare
• Power ranges vary depending on optic configuration; see website for complete information
For more information: http://www.rayner.com/en/sulcoflex

Courtesy of Rayner
Postoperatively, her UDVA was better than 20/20 in each eye, and she refracted to plano in her dominant eye and 0.25 D in her nondominant. Despite the fact that her corneal astigmatism was completely eliminated and her distance vision superb, she was highly troubled by the loss of her intermediate vision. I organized a 1-day trial of a 1.50 D soft contact lens in her nondominant eye to make her effectively -1.25 D in that eye (ie, mini-monivision). She tolerated this arrangement well and appreciated the restoration of her intermediate vision.
Her ocular surface, despite treatment, was too poor for hyperopic LASIK, so I elected a Sulcoflex implantation procedure, implanting a 2.50 D Sulcoflex in her nondominant eye (as determined by the Rayner online calculator) to make her mini-monovision permanent. She was happy with the outcome.
POINTERS AND PEARLS
Loading this sulcus lens into the injector and implanting it are straightforward procedures, well within the technical capability of general cataract surgeons. I ensure that there is some cohesive OVD in the sulcus prior to implantation, and I place the haptics of the Sulcoflex at 90° to the orientation of the haptics of the in-the-bag IOL.
I make sure to remove the OVD from between the two IOLs before completing the case (http://bit.ly/barsam0117).
Watch it Now
CONCLUSION
All of the Sulcoflex Pseudophakic Supplementary lenses provide a superb option for enhancing a less-than-satisfactory refractive outcome after cataract surgery. Having this option allows cataract surgeons to ensure that postoperative refractive outcomes can be adjusted and corrected in the relatively rare event that this is necessary.

