


My experience with small-aperture optics began with the Kamra corneal inlay (AcuFocus) for presbyopia. I have now participated in the evolution of this concept from the cornea to the lens plane, and I am excited about the performance of the IC-8 IOL (AcuFocus). I have implanted this lens in more than 50 eyes so far, with satisfactory results. The IOL is easy to use and manage, it has a broad range of applications, and it has proven, reliable optics.
DESIGN AND FUNCTION
The IC-8 is a one-piece hydrophobic acrylic IOL with an embedded black circular mask. The mask blocks unfocused rays of light, extending depth of focus and providing patients with good visual acuity across a range of distances. The lens is implanted in the nondominant eye, but it does not create monovision. Patients who receive the IC-8 IOL in one eye and a standard aspheric lens in the other have achieved an average UNVA of J1, along with 20/20 for both UIVA and UDVA.1 In another study, the small-aperture IOL did not decrease binocular contrast sensitivity, even under mesopic conditions.2
Unlike other premium lenses that require specific parameters to maximize their attributes, the IC-8 is an incredibly forgiving lens. It provides a broad range of functional vision with as much as ±1.00 D of deviation from the targeted manifest refraction spherical equivalent (MRSE). A deviation of more than 0.50 D from intended refractive target will result in a loss of 1 or 2 lines of vision with a typical monofocal or multifocal lens, but 100% of patients receiving the IC-8 IOL in clinical studies maintained 20/40 or better UDVA, even with refractive error ranging from 0.50 to -1.50 D.3
ADDRESSING ASTIGMATISM, REDUCING DYSPHOTOPSIA
In addition to its tolerance of residual refractive error, the pinhole effect of the IC-8 IOL also cancels the degradation of vision from up to 1.50 D astigmatism. According to a clinical study of 6,000 patients by Warren E. Hill, MD, 82% of the population has as much as 1.50 D cylinder prior to cataract surgery (personal communication). The IC-8 IOL provides a complete range of postoperative uncorrected visual acuity from near to far, including excellent distance vision, and compensates for the astigmatism in this group without the surgeon having to worry about performing precise refractive measurements, arcuate incisions, rotation of toric lenses, or other refractive procedures to correct postoperative residual error.
AT A GLANCE
• The embedded black circular mask of the IC-8 blocks unfocused rays of light to extend depth of focus and provide patients with good visual acuity across a range of distances.
• The pinhole effect of the IC-8 cancels the degradation of vision from up to 1.50 D astigmatism.
• The lens is implanted in the nondominant eye, but it does not create monovision.
Because this lens addresses these asymmetric problems with a symmetric optic, postrefractive measurements, preoperative eye marking, toric IOL alignment, and many uncontrolled factors such as surgically induced astigmatism or the impact of pupil size on vision are eliminated. For the majority of both regular and postkeratorefractive surgery patients with less that 1.50 D astigmatism, the IC-8 IOL is an excellent option.
The IC-8 IOL can also be beneficial in certain challenging cases. I have previously reported on a case in which a young man with ocular trauma that resulted in paracentral corneal perforation, a lenticular capsule defect, and iris defects received this lens.4 The anterior vitrectomy and corneal sutures performed for repair of the injury left him with a highly irregular cornea, and the patient complained of significant glare and photic phenomena.
The Lens: IC-8
ACUFOCUS
• Small-aperture principle provides continuous, uninterrupted range of vision
• Good quality night vision with few symptoms of glare and halos
• Compensates for up to 1.50 D astigmatism
• Biconvex 6-mm optic with square posterior edge
• Optic incorporates a nondiffractive 3.23-mm diameter opaque mask with a 1.36-mm central aperture
• One-piece hydrophobic acrylic IOL with modified–C haptics with 5° angulation
• Overall length 12.5 mm
• Available in powers of 15.50 to 27.50 D in 0.50 D steps
• Incision size of 3.5 mm with single-use injector

For more information: http://www.acufocus.com/int/sites/default/files/MK-1268%20Rev%20B%2C%20IC-8%20IOL%20Physician%20Brochure.pdf
At the time I operated on him, his visual acuity was 20/100, and Scheimpflug tomography measured him as having 1.40 D irregular astigmatism. I implanted the IC-8 IOL in the sulcus of the injured eye, and the small aperture, by allowing only the central, paraxial collimated light rays to reach the retina, reduced his photophobia. By 6 months after implantation, the patient had UDVA of 20/25 and UNVA of J3 for reading. He also reported minimal glare and light sensitivity at twilight and spectacle independence throughout the day.
A SIMPLIFIED PROCESS
The cataract surgical procedure when inserting the IC-8 IOL (Figure 1) is the same as for any other IOL, although perhaps simplified. It is still necessary to assess the patient’s astigmatism, but not to the same extent as with other lenses. The lens can be inserted through an incision of 3.2 to 3.5 mm. A video of laser-assisted cataract surgery with IC-8 implantation can be viewed at https://www.youtube.com/watch?v=rA25IyPzlC0".
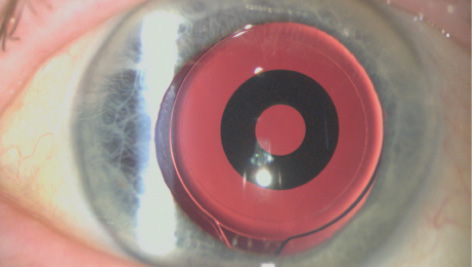
Figure 1. The IC-8 IOL in situ.
Most lenses use complex optical engineering to produce a desired visual outcome. The IC-8 IOL, on the other hand, uses the physics principle of the small aperture. Therefore, unless we somehow violate the laws of physics, this lens will work. It is an easy-to-use, symmetric solution for a broad range of patients that overcomes many of the challenges that surgeons may see with other premium IOLs.
1. Grabner G. Four decades of cataract surgery: personal visions for the future. Paper presented at: European Society of Cataract and Refractive Surgeons; September 13-17; London.
2. Manzanera S, Marin JM, Artal P. Contrast sensitivity with a small aperture IOL evaluated with an adaptive optics instrument. Paper presented at: European Society of Cataract and Refractive Surgeons; September 13-17; London.
3. Ang R. Visual and optical performance with a small aperture intraocular lens: first report. Paper presented at: European Society of Cataract and Refractive Surgeons; September 12, 2016; Copenhagen, Denmark.
4. Schultz T, Dick B. Small-aperture intraocular lens implantation in a patient with an irregular cornea. J Refract Surg. 2016;32(10):706-708.

