


In recent years, an array of new multifocal IOLs has emerged in response to the growing demands of presbyopic and cataract surgery patients for new lifestyle and visual needs. In particular, with the increasing use of digital devices such as computers, e-books, and smartphones, the ability to read at varying distances has taken on elevated importance.
Achieving optimal reading ability is essential, and this, in turn, will positively affect the patient’s perceived quality of life. Real-world reading is typically binocular, so it is essential to test reading vision binocularly and to use a standardized test to identify differences among multifocal IOL treatments.
AT A GLANCE
• The Diff-aA is capable of providing a full range of vision, including functional reading performance even under low illumination and contrast conditions.
• The author’s clinical experience suggests that this IOL can perform as well as one of the leading multifocal IOLs in the international marketplace.
The Salzburg Reading Desk-Advanced (SRD; SRD Vision) was developed for this purpose; it uses computerized testing under standardized conditions while simulating a natural reading process. The device received the CE Mark in 2012.
CLINICAL EXPERIENCE
At the Eye Clinic of the Paracelsus Medical University in Salzburg, my colleagues Alois Dexl, MD; Gerlinde Jell, MD; and I conducted a prospective randomized study comparing the visual outcomes and reading performance of two diffractive apodized multifocal IOLs: the Diffractiva Diff-aA +3.5 D (HumanOptics) and the AcrySof Restor +3.0 D (Alcon).
Both lenses have been designed to minimize visual disturbances and to have increasingly distance-dominant behavior as the pupil enlarges by changing the balance of energy distribution between distance and near images. However, the Diff-aA and the Restor +3.0 differ as follows, respectively: in their materials (hydrophilic vs hydrophobic), aspheric design (aberration-free vs aberration-correcting), near add power (3.50 vs 3.00 D), diameter of diffractive region (3.5 vs 3.6 mm), and apodization pattern.
Our study included 60 cataract surgery patients implanted with either the Diff-aA (n=30) or the Restor (n=30). Study outcomes were evaluated 3 months after surgery. Reading performance was evaluated at the patient-preferred reading distance under different luminance levels (100 cd/m2 and 20 cd/m2) and contrast conditions (95% and 30%).
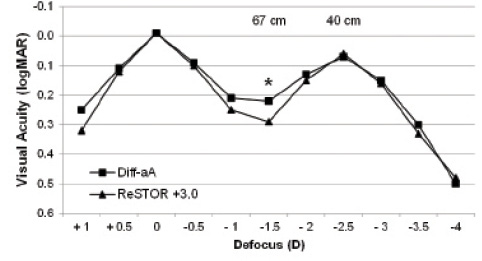
Figure 1. Defocus curves for the Diff-aA and the AcrySof Restor +3.0.
Both IOLs provided comparably good outcomes in terms of far visual acuity and reading performance under high luminance and contrast levels. The monocular defocus curves of the two IOLs (Figure 1) showed similar shapes, with maximum visual acuity at 0.00 D defocus for distance vision and at -2.50 D defocus at approximately 40 cm from the eye. However, we found significantly better visual acuity at -1.50 D of defocus (approximately 67 cm from the eye) in the Diff-aA group (P=.01). Nonetheless, both IOLs provided a good range of vision from near to far, with comfortable intermediate vision. This is in agreement with published reports.1,2
A key finding of this study was overall better reading performance in the Diff-aA group under low luminance and contrast levels. Both study groups had similar pupil sizes under mesopic conditions, so pupil size could not be a factor in these results. Furthermore, we found no correlation between pupil size and any of the reading parameters measured. Therefore, we believe that the most plausible explanation for the discrepancy is the difference in the optical quality of the two lens materials, as explained in more detail below.
The Lens: Diffractiva Diff-aA
HUMANOPTICS
• One-piece hydrophilic acrylic material with UV absorber
• Aberration-free aspheric anterior surface
• Diffractive multifocal with 3.50 D add at IOL plane
• Posterior surface with 360° lens epithelial cell barrier
• UV-absorbing, with blue light protection optional (Diff-aAY)
• Sphere power 10.00 to 30.00 D in 0.50 D steps
For more information: https://www.humanoptics.com/en/surgeons/products/intraocularlenses/diffractiva.html

Courtesy of HumanOptics
Frequency of spectacle wear was low in both groups (Figure 2), with slightly better outcomes in the Diff-aA group. As expected, we found that most patients experienced halos and glare both pre- and postoperatively. The preoperative versus postoperative difference in disturbance score for halos (slightly higher postoperatively) was more pronounced in the Restor group than in the Diff-aA group (P=.02 vs P=.09). In both groups, the glare disturbance score decreased significantly postoperatively (Diff-aA group, P=.01; Restor group, P=.03). Overall, patient satisfaction scores were high in both groups, and no patient reported being “not at all satisfied.”
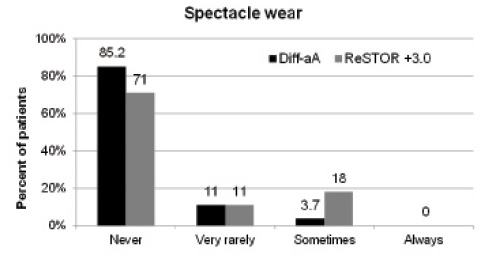
Figure 2. Postoperative spectacle wear with the two lenses.
ADVANTAGES OF THE DIFF-aA DESIGN
Hydrophilic IOLs tend to be easier for the surgeon to implant than hydrophobic IOLs. We started using the Diff-aA shortly after its launch in September 2010 and have observed a low incidence of posterior capsular opacification, which is possibly related not only to surgical technique but also to the true 360° posterior edge of the lens optic.
Advantage No. 1: Lens material. The key advantage of the Diff-aA, however, seems to be the exceptional quality of the lens material, which, we feel, might explain the better performance of the lens under mesopic conditions compared with the Restor. It is well accepted that chromatic aberrations impact negatively on vision, particularly on contrast sensitivity.3 Each implant has a fixed level of chromatic aberration, indicated by its Abbe number, which is intrinsic to the lens material itself: the higher, the better. With Abbe numbers of 57 for the Diff-aA material and age quality.
Advantage No. 2: The aberration-free design. With this design, the Diff-aA is somewhat immuecting IOLs.
Advantage No. 3: Apodization pattern. Finally, the apodization pattern of the Diff-aA seems to provide better intermediate vision than one might have expected from a multifocal IOL with a purely bifocal design.
POINTERS AND PEARLS
The Diff-aA is a versatile lens that can provide good visual function across a range of distances. However, this multifocal IOL seems particularly ideal for patients who demand functional reading performance under dim light conditions.
One of the main drivers for optimal patient satisfaction after multifocal IOL implantation is spectacle independence. Therefore, accurate calculation of IOL power for all eyes is essential to avoid postoperative refractive errors. In general, each manufacturer’s formula constants are good starting points, but they do not guarantee perfect outcomes for an individual. I recommend that surgeons optimize their A-constants to come closer to their intended target refractions. Using our set of Diff-aA refractive data, IOL constant optimization was performed using the online service provided by Wolfgang Haigis, PhD. The optimized constants are available at: http://www.ocusoft.de/ulib/c1.htm.
1. Dexl AK, Zaluski S, Rasp M, Grabner G. Visual performance after bilateral implantation of a new diffractive aspheric multifocal intraocular lens with a 3.5 D addition. Eur J Ophthalmol. 2014;24(1):35-43.
2. Kohnen T, Nuijts R, Levy P, Haefliger E, Alfonso JF. Visual function after bilateral implantation of apodized diffractive aspheric multifocal intraocular lenses with a +3.0 D addition. J Cataract Refract Surg. 2009;35(12):2062-2069.
3. Zhao H, Mainster MA. The effect of chromatic dispersion on pseudophakic optical performance. Br J Ophthalmol. 2007;91(9):1225-1229.

