




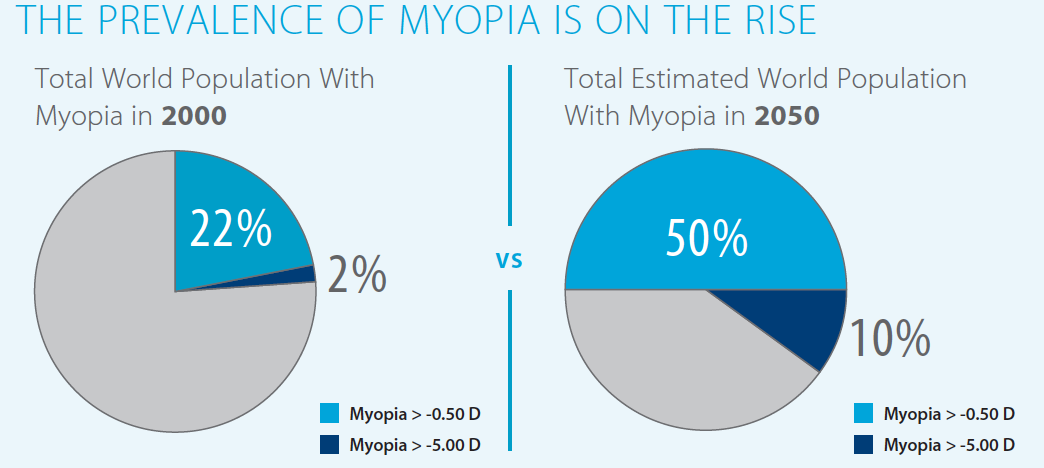
Myopia is the most common cause of correctable vision loss in the world, and it continues to increase in prevalence. It is estimated that, by 2050, 50% of the world, or 5 billion people, will have myopia greater than -0.50 D, compared with 22% in 2000, and 10%, or 1 billion people, will have myopia greater than -5.00 D, compared with 2% in 2000.1
Myopia can lead to numerous secondary problems, including myopic retinal degeneration and retinal detachment, and it can significantly affect an individual’s quality of life. Overall, this is a topic of concern well known to optometrists but less commonly discussed in the ophthalmology community. The importance of myopia prevention efforts was introduced to us 7 years ago at the Eye & Contact Lens Association (CLAO) Annual Meeting.
Both genetic and environmental factors influence the development of myopia. Furthermore, theories around the progression of myopia have been based on the concept of peripheral hyperopic defocus. A variety of treatments have been studied in efforts to both delay the onset of myopia and to slow its progression.
ENVIRONMENTAL INFLUENCES
The greatest modifiable environmental factor in the development of myopia appears to be time spent outdoors. The Sydney Myopia Study found that children with low amounts of outdoor activity and high amounts of near-work activity had two- to threefold higher odds for myopia than children with high outdoor and low near-work activity levels.2
Two theories have been proposed to explain these results. First, higher light intensities outdoors lead to more constricted pupils and therefore greater depth of field and less image blur. Second, light stimulates release of dopamine from the retina, which acts as an inhibitor of eye growth. Interestingly, increasing outdoor activity has been found to delay the onset of myopia but does not slow its progression.3,4
REFRACTIVE CORRECTION
Refractive error correction methods for slowing the progression of myopia are centered around reducing relative retinal peripheral hyperopia. This is based on the concept that myopic individuals have a relative hyperopic defocus in the retinal periphery due to their longer axial lengths, and this peripheral blurring is a greater stimulus for eye growth than central blurring.4 Multifocal or bifocal spectacle lenses and peripheral defocus–modifying contact lenses have been used in efforts to combat this effect. Overall, studies of multifocal spectacles have shown differing effects, whereas contact lenses that modify peripheral defocus were found to be a superior method of correction.5
Orthokeratology has also been shown to be effective in controlling the progression of myopia. These specialized rigid contact lenses are designed to be worn at night to reshape the cornea and correct refractive error so that patients can be free of correction during the day. The lenses flatten the central cornea and steepen the midperipheral cornea, thereby reducing peripheral hyperopia.5 Orthokeratology is a viable option in myopia control, as long as the lenses are fit carefully and the patient and his or her family understand proper care and cleaning of the lenses. With education and compliance, the complication rate in the United States (including infection) is acceptably low.6 The cost to the patient is around US$1,000 to US$2,000 for lenses, examination, and follow-up fitting appointments.
PHARMACOLOGIC THERAPY
Antimuscarinic agents such as atropine have been shown to reduce the progression of myopia, although their exact mechanism of action is largely unknown. Studies conducted in Singapore by Tan and colleagues have been paramount in increasing our understanding of the use of atropine for myopia.7 The first Atropine for the Treatment of Myopia (ATOM1) trial found that daily use of topical atropine 1% led to a 77% reduction in myopia progression compared with placebo.8 A second trial, ATOM2, then compared atropine in weaker concentrations (0.5%, 0.1%, 0.01%) and found that the effect of myopia control was dose-dependent, but the differences between groups were clinically small.9 Furthermore, the decreased ocular side effect profile of the lowest dose, 0.01% atropine, made it the most favorable option.
Further phases of the ATOM2 trial demonstrated that the rebound effect after stopping atropine was lowest in the 0.01% group10 and that, if progression was significant enough to require restarting therapy, the original 0.01% group had the least progression.11 Additional studies by Fang et al using atropine 0.025% found a statistically significant difference in the onset of myopia (21% in the treatment group vs 54% in the control group).12
CONCLUSION
Myopia prevention efforts appear to work. Increasing time spent outdoors may delay the onset of myopia, and treatment with atropine may slow myopic progression. In addition to low-dose atropine (0.01%), other effective and practical methods to decrease progression of myopia include soft contact lenses with peripheral defocus–modifying designs, and orthokeratology.
To learn more about myopia prevention efforts, join CLAO (https://www.clao.org/).
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042.
2. Rose KA, Morgan IG, Ip J, Kifley A. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279-1285.
3. Walline JJ. Myopia control: a review. Eye Contact Lens. 2016;42(1):3-8.
4. Warner N. Update on myopia. Curr Opin Ophthalmol. 2016;27(5):402-406.
5. Huang J, Wen D, Wang Q, et al. Efficacy comparison of 16 interventions for myopia control in children: a network meta-analysis. Ophthalmology. 2016;123(4):697-708.
6. Liu YM, Xie P. The safety of orthokeratology—a systematic review. Eye Contact Lens. 2016;42(1):35-42.
7. Tan D, Tay SA, Loh K-L, Chia A. Topical atropine in the control of myopia. Asia-Pacific J Ophthalmol. 2016;5(6):424-428.
8. Chua WH, Balakrishnan V, Chan YH, et al. Atropine for the treatment of childhood myopia. Ophthalmology. 2006;113(12):2285-2291.
9. Chia A, Chua WH, Cheung YB, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012;119(2):347-354.
10. Chia A, Chua WH, Wen L, Fong A, Goon YY, Tan D. Atropine for the treatment of childhood myopia: Changes after stopping atropine 0.01%, 0.1% and 0.5%. Am J Ophthalmol. 2014;157(2):451-457.e1.
11. Chia A, Lu QS, Tan D. Five-year clinical trial on atropine for the treatment of myopia 2 myopia control with atropine 0.01% eyedrops. Ophthalmology. 2016;123(2):391-399.
12. Fang P-C, Chung M-Y, Yu H-J, Wu P-C. Prevention of myopia onset with 0.025% atropine in premyopic children. J Ocul Pharmacol Ther. 2010;26(4):341-345.