




As lifespans around the world have gotten longer, the pseudophakic population has grown. Further, the indications for cataract surgery have expanded as a result of the excellent outcomes and high predictability of the technique. Despite these successes, complications do arise, and, over the past few years, the number of published reports about IOL explantation has grown significantly.1
AT A GLANCE
- Over the past few years, the number of published reports about IOL explantation has grown significantly.
- Multifocal IOL explantation in dissatisfied patients is a feasible option that can significantly improve patient satisfaction and visual acuity.
- IOL exchange is not devoid of complications, so it is important to rule out all causes of poor quality of vision before considering IOL explantation surgery.
- The authors expect to see an increasing number of IOL explantation surgeries in the coming years, especially due to late IOL dislocation.
This article reviews five fundamental points about IOL explantation, when it may be needed, and how it should be approached.

There are multiple causes of IOL explantation
In a long-term retrospective study, Jin et al found an overall rate of IOL explantation of 0.77%.2 In separate investigations, Jakobsson et al and Clark et al reported that the incidence of surgery specifically due to late IOL dislocation was 0.032% to 0.28%.3,4
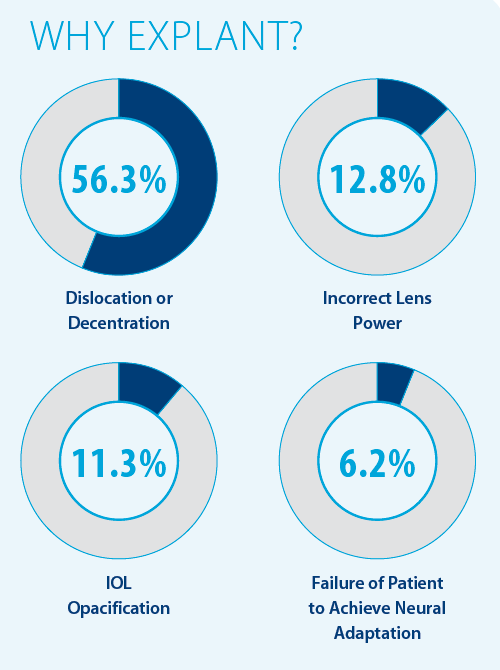
Our research group published a study that looked at 257 explanted pseudophakic IOLs.5 The main causes for explantation were dislocation or decentration, incorrect lens power, IOL opacification, and failure to neurally adapt (see Why Explant? below). Incorrect lens power and failure to neurally adapt to multifocal IOLs are well recognized indications for IOL explantation and exchange. There was an epidemic of IOL opacification in the past, especially associated with certain IOL models, but it still occurs even with some new IOL models.

IOL dislocation is the most common cause of explantation
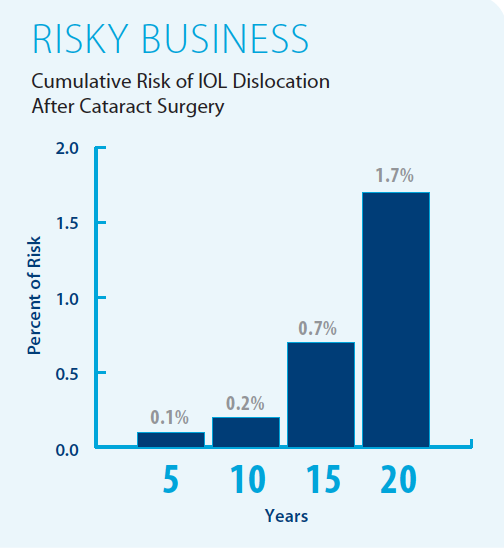
In an observational study, the cumulative risk of IOL dislocation varied according to the number of years after cataract extraction (see Risky Business below).6 The risk factors for this condition include pseudoexfoliation (PXF), connective tissue disorders, uveitis, retinitis pigmentosa, high myopia, and a history of vitreoretinal surgery.
Although PXF is probably the most well-recognized predisposing factor for late dislocation, its incidence depends greatly on geographic location. A study by our research group found that high myopia was the most prevalent risk factor, followed by PXF.7 Patients in the high myopia group were younger at the time of explantation than patients in the PXF group (P = .001). In that report, the mean time interval from cataract surgery to explantation due to late dislocation was 7.5 ±5.2 years. Other reports have shown mean intervals of around 8 years.3

Despite advances in cataract surgery, unsatisfactory visual outcomes as a result of a residual refractive error still occur
In a recent report analyzing refractive data from more than 17,000 eyes after cataract surgery, emmetropia was attained in only 55% of eyes targeted for it.8
The options to correct unwanted refractive outcomes include laser- and lens-based procedures (LASIK or PRK for the former, IOL exchange or piggyback IOL implantation for the latter). Fernández-Buenaga et al conducted a retrospective comparison of LASIK, piggyback IOL, and IOL exchange as methods to correct residual refractive error.9 All three methods were capable of improving refraction in myopic and hyperopic eyes. The study found that LASIK was the most accurate and predictable procedure for correction of residual ametropia after cataract surgery. Lens-based procedures (IOL explantation or piggyback) are also effective, and they should be preferred in eyes with extreme ametropia or corneal abnormalities and when no excimer laser platform is available.
The proportion of eyes that lost one or more lines of BCVA was four to five times higher in the IOL explantation and piggyback groups than in the LASIK group.9

IOL opacification is a relatively old problem, but it can still occur
Recent reports show that calcification can still occur in hydrophilic IOLs in association with certain conditions, such as a history of gas use in the eye.10 Calcification has been described in a relatively recently introduced hydrophilic IOL with a hydrophobic surface in association with medical conditions including diabetes, hypertension, and glaucoma.11
IOL opacification usually leads to decreased visual acuity and poor quality of vision, with high levels of light scattering and decreased contrast sensitivity. Hence, the decision to explant should be based on clinical examination findings combined with documentation of decreased visual acuity or quality of vision.
Most published papers show a long interval between cataract surgery and IOL exchange due to opacification. In a retrospective study by our group, we found an average interval of 89.1 ±33.6 months from primary surgery to IOL explanation due to opacification.12 A final BCVA of 0.7 or better was achieved in 68.2% of these eyes.
In that study, IOL exchange was uneventful in most cases; however, it is not exempt from complications. Anterior vitrectomy had to be performed in almost one-third of the eyes, and the new IOL had to be implanted in the ciliary sulcus in many patients (63.6%).

Some multifocal IOL patients fail to achieve neural adaptation
Multifocal IOL explantation is the worst scenario possible after cataract surgery with multifocal IOL implantation for two reasons: (1) it is a separate surgical event that can be associated with new complications, and (2) it means that the aim of the original surgery was missed. Fortunately, it is needed in only a few patients. Studies have reported rates of multifocal IOL exchange among dissatisfied patients ranging from 0.85% to 7%.13,14
Explantation surgery is always challenging, but explantation of a multifocal lens is usually easier (especially with a capsular tension ring) than explantation due to other causes. This is because, first, the decision to explant is made only few months after the cataract surgery, when scarring has not yet occurred, and second, the surgery is less risky because no ocular structures are damaged.
Kamiya et al conducted a retrospective study including 50 eyes that required multifocal IOL explantation.13 Patient satisfaction for overall quality of vision was graded on a scale of 1 (very dissatisfied) to 5 (very satisfied). After IOL exchange surgery, patient satisfaction was significantly increased, from 1.22 ±0.55 preoperatively to 3.78 ±0.98 postoperatively.
Anterior vitrectomy was necessary in three cases in that series (6%). The IOL was placed in the bag in 38 eyes (76%) and in the sulcus in 11 eyes (22%). Sulcus placement with scleral suturing was required in one eye (2%).
CONCLUSION
Multifocal IOL explantation in dissatisfied patients is a feasible option that can significantly improve patient satisfaction and quality of vision.
Multifocal IOL exchange is not devoid of complications, so it is important to rule out all causes of poor quality of vision (eg, dry eye, IOL decentration, residual refractive error, posterior capsular opacification) before considering IOL explantation surgery. It is important to perform specific tests to accurately assess visual function, especially in patients with good visual acuity who nonetheless complain of poor vision. Decreased contrast sensitivity is found in most of these cases.15
We expect to see an increasing number of IOL explantation surgeries in the coming years, especially due to late IOL dislocation. It is essential for anterior segment surgeons to know the causes that can lead to explantation, to recognize the risk factors, to explain to patients the prognosis for the surgery, and to perform the explantation technique that is best for each patient.
1. Fernandez-Buenaga, Alió JL. Intraocular lens explantation after cataract surgery: indications, results, and explantation techniques. Asia Pac J Ophthalmol. 2017;6(4):372-380.
2. Jin GJ, Crandall AS, Jones JJ. Changing indications for and improving outcomes of intraocular lens exchange. Am J Ophthalmol. 2005;140(4):688-694.
3. Jakobsson G, Zetterberg M, Lundstrom M, et al. Late dislocation of in-the-bag and out-of-the bag intraocular lenses: ocular and surgical characteristics and time to lens repositioning. J Cataract Refract Surg. 2010;36(10):1637-1644.
4. Clark A, Morlet N, Ng JQ, et al. Whole population trends in complications of cataract surgery over 22 years in western Australia. Ophthalmology. 2011;118(6):1055-1061.
5. Fernández-Buenaga R, Alio JL, Muñoz-Negrete FJ, et al. Causes of IOL explantation in Spain. Eur J Ophthalmol. 2012;22(5):762-768.
6. Pueringer SL, Hodge DO, Erie JC. Risk of late intraocular lens dislocation after cataract surgery, 1980-2009: a population-based study. Am J Ophthalmol. 2011;152:618-623.
7. Fernández-Buenaga R, Alio JL, Pérez-Ardoy AL, et al. Late in-the-bag intraocular lens dislocation requiring explantation: risk factors and outcomes. Eye (Lond). 2013;27(7):795-801.
8. Behndig A, Montan P, Stenevi U, et al. Aiming for emmetropia after cataract surgery: Swedish National Cataract Register study. J Cataract Refract Surg. 2012;38:1181-1186.
9. Fernández-Buenaga R, Alió JL, Pérez Ardoy AL, et al. Resolving refractive error after cataract surgery: IOL exchange, piggyback lens, or LASIK. J Refract Surg. 2013;29(10):676-683.
10. Dhital A, Spalton DJ, Goyal S, et al. Calcification in hydrophilic intraocular lenses associated with injection of intraocular gas. Am J Ophthalmol. 2012;153:1154-1160.
11. Bompastor-Ramos P, Póvoa J, Lobo C, et al. Late postoperative opacification of hydrophilic-hydrophobic acrylic intraocular lens. J Cataract Surg. 2016;42:1324-1331.
12. Fernández-Buenaga R, Alió JL. Pinilla-Cortés L, et al. Perioperative complications and clinical outcomes of intraocular lens exchange in patients with opacified lenses. Graefes Arch Clin Exp Ophthalmol. 2013;251:2141-2146.
13. Venter JA, Pelouskova M, Collins BM, et al. Visual outcomes and patient satisfaction in 9366 eyes using a refractive segmented multifocal intraocular lens. J Cataract Refract Surg. 2013;39(10):1477-1484.
14. Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992-997.
15. Kamiya K, Hayashi K, Shimizu K, et al. Multifocal intraocular lens explantation: a case series of 50 eyes. Am J Ophthalmol. 2014;158:215-220.
